03
Introduction
Background of the project
Uganda has, over the past decades, emerged as one of the most significant refugee-hosting countries globally, driven by its progressive refugee policies and its geographical proximity to countries experiencing protracted conflict and instability. The country’s open-door policy, enshrined in the Refugees Act (2006) and Refugee Regulations (2010), has allowed refugees access to land, public services, and freedom of movement. While this approach has been widely recognized as a model for refugee inclusion, it has simultaneously placed considerable pressure on already constrained national systems, particularly in the health and protection sectors.
The project “Protecting the dignity of refugees in Uganda: responding to sexual and gender-based violence as a human rights violation and public health issue” was designed within this complex humanitarian context. It built on over five years of collaboration between Farmacéuticos Mundi (Farmamundi), Africa Humanitarian Action (AHA), and Emesco Development Foundation (EMESCO), organizations that had jointly implemented multiple health and protection interventions targeting refugee populations in Uganda. The project represented a continuation and consolidation of previous initiatives, incorporating lessons learned from earlier programmes to strengthen both the quality and scope of humanitarian response.
The aim of the intervention was to contribute to the promotion of the right to health and the right to live with dignity among refugee populations, with a specific focus on addressing sexual and gender-based violence (SGBV) as both a human rights violation and a critical public health concern. The project was based on the recognition that the vulnerabilities experienced by refugees are multidimensional, stemming not only from displacement but also from systemic inequalities, limited access to services, and exposure to violence—particularly for women and girls.
The intervention was implemented across three distinct geographic contexts, Kampala (urban), Kyaka II (rural settlement), and Adjumani (large-scale settlement in northern Uganda), each characterized by unique demographic, socio-economic, and health-related challenges. This multi-site approach reflected the understanding that refugee experiences in Uganda were not homogeneous, and that tailored strategies were required to address both urban and settlement-specific vulnerabilities.
At its core, the project was grounded in a rights-based and integrated approach, linking healthcare delivery with gender equality, protection, and community empowerment. It aimed not only to improve access to essential health services but also to strengthen the capacity of communities and institutions to prevent and respond to SGBV, while fostering accountability and participation among affected populations. This approach aligned with international humanitarian standards, including the Core Humanitarian Standard (CHS), and emphasized the importance of transparency, responsiveness, and inclusiveness in service delivery.
The project was structured around a specific objective and a set of interconnected results aimed at improving both service provision and systemic capacity. The specific objective focused on enhancing the health and sexual and reproductive health (SRH) of refugee populations by addressing SGBV through a comprehensive, multisectoral response. This included improving access to primary healthcare services, strengthening mental health and psychosocial support (MHPSS), enhancing referral systems for specialized care, and ensuring that survivors of violence received adequate medical, psychological, and legal support.
One of the central pillars of the intervention was the expansion of access to essential healthcare services, particularly in underserved refugee settings. Prior to the project, access to healthcare had been constrained by multiple barriers, including long distances to health facilities, insufficient medical supplies, understaffing, and high demand resulting from increasing refugee influxes. The project sought to address these gaps through a combination of facility-based services and mobile outreach teams, ensuring that both static and hard-to-reach populations could benefit from healthcare interventions.
In addition to healthcare delivery, the project placed significant emphasis on mental health and psychosocial support (MHPSS). Refugee populations were often exposed to traumatic experiences, including conflict-related violence, displacement, and loss of livelihoods, all of which contributed to a high burden of mental health conditions. Despite this, mental health services in many humanitarian settings remained limited. The project addressed this gap by integrating psychosocial support into primary healthcare services and deploying mobile teams to provide community-based support, thereby increasing both the availability and accessibility of care.
Another component of the intervention was the strengthening of referral systems to ensure that refugees requiring specialized medical services could access appropriate care at higher-level facilities, including national referral hospitals in Kampala. This was particularly important for cases involving complex medical conditions or survivors of SGBV who required comprehensive support. The project therefore reinforced coordination between primary healthcare providers and tertiary institutions, facilitating timely and effective referrals.
Capacity building of healthcare professionals and stakeholders was another area. The project included targeted training programmes aimed at enhancing the technical skills of healthcare workers, particularly in areas such as SGBV response, mental health care, and adherence to standardized treatment protocols. By strengthening the knowledge and competencies of service providers, the intervention contributed to improved quality of care and ensured that services were delivered in a manner that was sensitive to gender and human rights considerations.
Beyond service delivery, the project recognized the importance of community engagement and awareness-raising in addressing the root causes of vulnerability. Activities were therefore designed to increase knowledge and awareness among refugee populations and host communities regarding health rights, gender equality, and the prevention of violence. These efforts aimed to challenge harmful social norms, reduce stigma associated with SGBV, and empower individuals, particularly women and girls, to seek services and assert their rights.
The intervention also incorporated mechanisms to strengthen accountability and participation, ensuring that affected populations had a voice in the design and implementation of activities. Feedback systems, community dialogues, and coordination structures were utilized to promote transparency and responsiveness, in line with the principles of the Core Humanitarian Standard. This participatory approach not only enhanced the relevance of interventions but also contributed to building trust between communities and service providers.
Importantly, the project operated within a broader humanitarian ecosystem, complementing the efforts of government institutions, UN agencies, and other non-governmental organizations. It did not aim to replace national systems but rather to support and strengthen them, particularly in areas where gaps in service delivery and protection persisted. This collaborative approach was essential given the scale and complexity of the refugee crisis in Uganda, where no single actor could address all needs.
Uganda refugee context
Uganda has consistently been among the largest refugee-hosting countries in the world and remains the largest in Africa. Its progressive refugee policy framework, which promotes inclusion and self-reliance, has enabled the country to host large numbers of refugees fleeing conflict, insecurity, and persecution in neighbouring countries, particularly South Sudan, the Democratic Republic of Congo (DRC), and Somalia. This long-standing commitment has positioned Uganda as a key actor in the global refugee response, with its refugee population has been steadily increasing over the past fifteen years. However, this has also placed significant strain on national systems and local resources.
: Refugee population increase - OPM
At the time of project implementation, Uganda was hosting over 1.5 million refugees, with the majority originating from South Sudan and the DRC. Refugee populations were unevenly distributed across the country, with large concentrations in settlement areas such as Adjumani in Northern Uganda and Kyaka II in Western Uganda, alongside a significant and growing number of refugees residing in urban settings, particularly Kampala.
The refugee situation in Uganda was characterized by a protracted crisis, with many refugees living in the country for extended periods due to ongoing instability in their countries of origin. This prolonged displacement resulted in increased dependency on humanitarian assistance and limited opportunities for sustainable livelihoods. At the same time, the continuous influx of new arrivals further exacerbated pressure on already overstretched services and infrastructure.
Despite Uganda’s inclusive policy framework, refugees continued to face multiple barriers in accessing essential services. The health system, in particular, struggled to cope with increased demand, especially in areas hosting large refugee populations. Health facilities often experienced shortages of medicines, limited human resources, and insufficient infrastructure, which compromised the quality and continuity of care. These challenges were further compounded in remote settlement areas, where geographical barriers and limited transport options restricted access to health services.
Access to sexual and reproductive health (SRH) and mental health and psychosocial support (MHPSS) services remained particularly constrained. While some services were available, their coverage and quality varied significantly across locations. Baseline findings indicated that satisfaction with SRH services was below optimal levels in all intervention areas, while MHPSS services were even more limited, particularly in settlement contexts. This highlighted systemic gaps in service delivery and emphasised the need for targeted interventions to strengthen both access and quality of care.
Gender-based violence (GBV) represented one of the most critical protection concerns within refugee communities. The prevalence of GBV was significant across all intervention areas, with multiple forms of violence including physical, emotional, and sexual violence—reported among refugee populations. Women and girls were disproportionately affected, often facing heightened vulnerability due to economic dependency, social norms, and limited access to protection services. At the same time, stigma, fear of retaliation, and weak reporting mechanisms contributed to underreporting and limited access to support services.
The response to GBV was further constrained by systemic challenges, including gaps in coordination between health, legal, and psychosocial services, as well as limited capacity of service providers to deliver comprehensive, survivor-centred care. While referral pathways existed, their effectiveness was often undermined by logistical barriers, lack of awareness, and insufficient integration across sectors.
In addition to health and protection challenges, refugee populations faced significant socio-economic vulnerabilities. Limited livelihood opportunities, food insecurity, and inadequate access to education and social services contributed to a cycle of dependency and vulnerability. Women, adolescents, persons with disabilities, and older persons were particularly affected, often experiencing compounded barriers to access and participation.
The context also revealed important gaps in awareness and knowledge among refugee populations regarding their rights, available services, and mechanisms for seeking support. Although there were ongoing efforts to promote health education and community engagement, these remained insufficient to address deeply rooted social norms and behavioural barriers, particularly in relation to gender equality and GBV.
At the community level, participation and accountability mechanisms were still evolving. While structures such as community dialogues and coordination committees were in place, their functionality and inclusiveness varied across locations. Strengthening these mechanisms was therefore essential to ensure that interventions remained responsive to the needs and priorities of affected populations and aligned with humanitarian accountability standards.
The three areas of intervention, Kampala, Kyaka II, and Adjumani, presented distinct contextual dynamics that influenced both the design and implementation of the project. Kampala, as an urban setting, was characterized by dispersed refugee populations, higher cost of living, and challenges related to access to affordable services and livelihoods. Refugees in urban areas often relied on public health facilities, which were not specifically tailored to refugee needs, and faced additional barriers such as discrimination, lack of documentation, and limited social support networks.
In contrast, Kyaka II and Adjumani represented settlement-based contexts, where refugees were hosted in designated areas with access to humanitarian services. While these settings allowed for more structured service delivery, they were also marked by challenges related to overcrowding, limited infrastructure, and dependence on external support. In Adjumani, the high concentration of refugees placed additional pressure on local resources, while in Kyaka II, geographical spread and access constraints further complicated service delivery.
Across all three locations, the refugee context was further shaped by broader systemic challenges, including funding gaps, coordination constraints, and the limitations of short-term humanitarian programming. These factors underscored the need for integrated, sustainable, and context-sensitive interventions that could address both immediate needs and longer-term structural challenges.
Overview of intervention areas (Kyaka II, Kampala, Adjumani)
 The project was implemented
across three distinct locations in Uganda, Kyaka II refugee settlement,
Kampala (urban), and Adjumani refugee settlements, each representing
different dimensions of the refugee experience in the country. Possibly,
these locations were strategically selected to capture the diversity of
refugee contexts in Uganda and to ensure that the intervention responded
to both settlement-based and urban challenges.
The project was implemented
across three distinct locations in Uganda, Kyaka II refugee settlement,
Kampala (urban), and Adjumani refugee settlements, each representing
different dimensions of the refugee experience in the country. Possibly,
these locations were strategically selected to capture the diversity of
refugee contexts in Uganda and to ensure that the intervention responded
to both settlement-based and urban challenges.
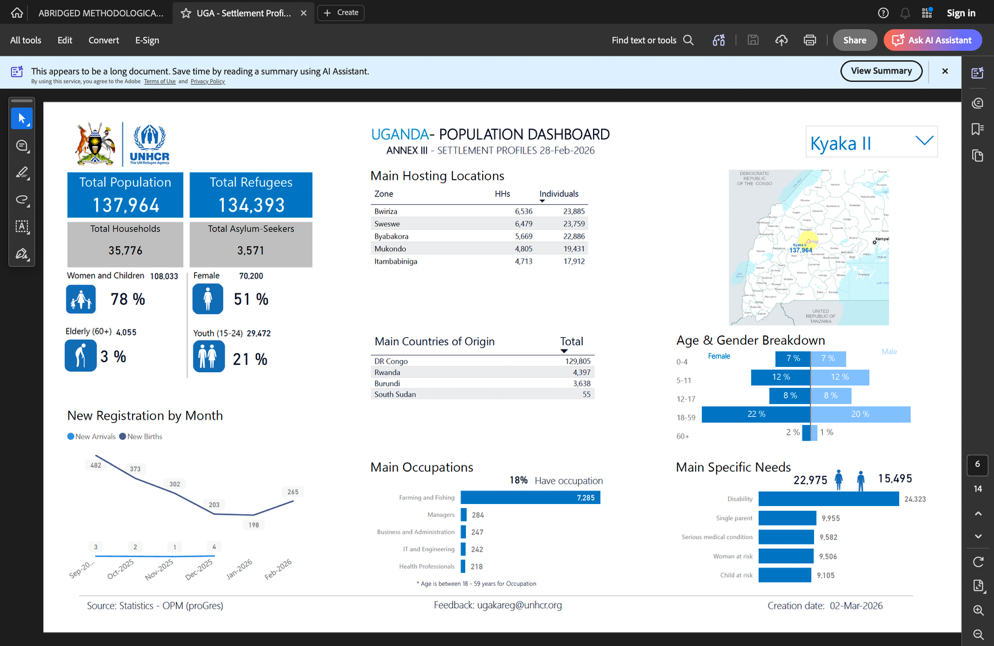
Kyaka II Refugee Settlement, located in Kyegegwa District in Western Uganda, hosts a predominantly Congolese refugee population. The settlement is characterized by a dispersed population across a wide geographic area, with limited infrastructure and significant barriers to accessing essential services. Health facilities in Kyaka II often face high patient loads, shortages of medicines, and limited human resources, which affect the quality and timeliness of care. Additionally, long distances between communities and health facilities, combined with limited transport options, further constrain access to services. These challenges are particularly pronounced for vulnerable groups, including women, children, and persons with disabilities. The context in Kyaka II is therefore largely defined by constraints in physical access, resource availability, and service capacity.
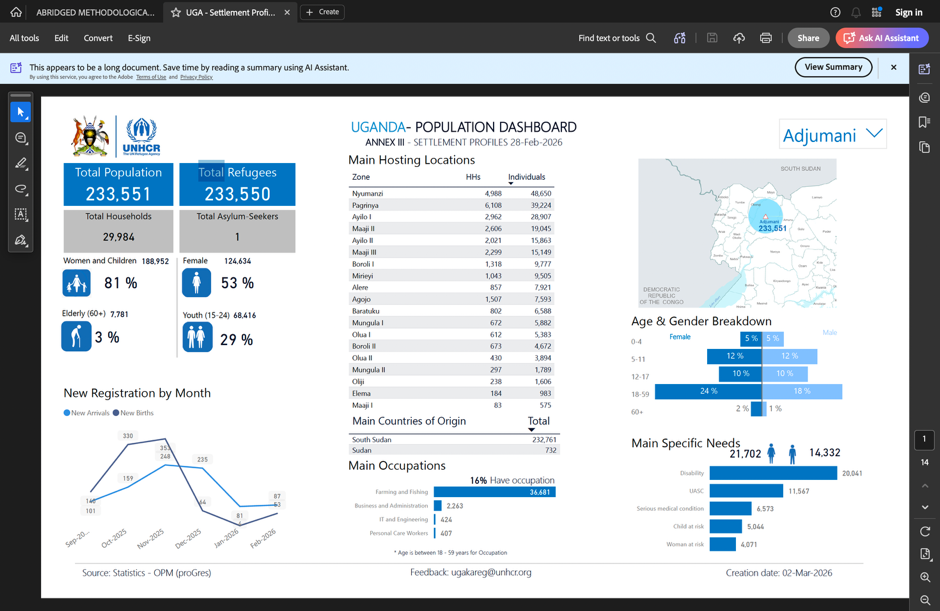 Adjumani
Settlements, located in Northern Uganda, is one of the largest
refugee-hosting districts in the country, hosting a significant
population of refugees, primarily from South Sudan. Unlike Kyaka II,
Adjumani is characterized by a high concentration of refugees within
relatively defined settlement areas. While this allows for more
structured service delivery and coordination among humanitarian actors,
the sheer scale of the refugee population places considerable pressure
on existing infrastructure and public services. Health facilities often
experience overcrowding, and the demand for services frequently exceeds
available capacity. In addition, protection concerns, including
gender-based violence, are prevalent, and access to comprehensive,
multisectoral services remains inconsistent. The Adjumani context is
therefore shaped by high demand, resource strain, and the complexities
of managing large-scale humanitarian operations.
Adjumani
Settlements, located in Northern Uganda, is one of the largest
refugee-hosting districts in the country, hosting a significant
population of refugees, primarily from South Sudan. Unlike Kyaka II,
Adjumani is characterized by a high concentration of refugees within
relatively defined settlement areas. While this allows for more
structured service delivery and coordination among humanitarian actors,
the sheer scale of the refugee population places considerable pressure
on existing infrastructure and public services. Health facilities often
experience overcrowding, and the demand for services frequently exceeds
available capacity. In addition, protection concerns, including
gender-based violence, are prevalent, and access to comprehensive,
multisectoral services remains inconsistent. The Adjumani context is
therefore shaped by high demand, resource strain, and the complexities
of managing large-scale humanitarian operations.
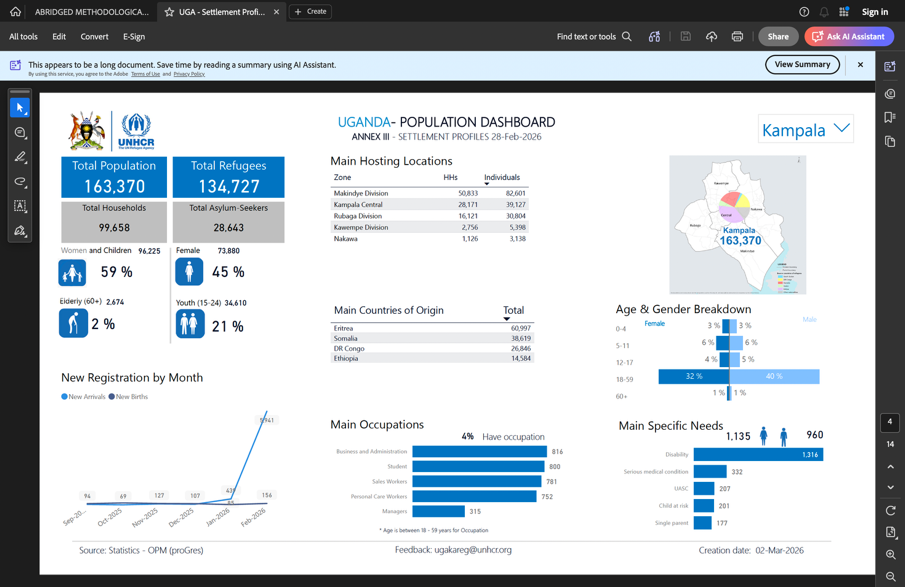 Kampala, as
the capital city and primary urban centre of Uganda, presents a markedly
different context from settlement areas. Refugees in Kampala are
dispersed across the city and are integrated within host communities
rather than residing in designated settlements. While urban settings
offer relatively better access to infrastructure and specialized
services, refugees face distinct challenges related to affordability,
documentation, discrimination, and limited social support systems.
Access to healthcare services is often constrained by cost, and refugees
must rely on public health facilities that are not specifically tailored
to their needs. Additionally, the identification and targeting of
vulnerable populations in urban settings is more complex due to the
absence of centralized settlement structures. The Kampala context is
therefore characterized by issues of invisibility, economic
vulnerability, and fragmented access to services.
Kampala, as
the capital city and primary urban centre of Uganda, presents a markedly
different context from settlement areas. Refugees in Kampala are
dispersed across the city and are integrated within host communities
rather than residing in designated settlements. While urban settings
offer relatively better access to infrastructure and specialized
services, refugees face distinct challenges related to affordability,
documentation, discrimination, and limited social support systems.
Access to healthcare services is often constrained by cost, and refugees
must rely on public health facilities that are not specifically tailored
to their needs. Additionally, the identification and targeting of
vulnerable populations in urban settings is more complex due to the
absence of centralized settlement structures. The Kampala context is
therefore characterized by issues of invisibility, economic
vulnerability, and fragmented access to services.
Across all three locations, refugee populations faced common challenges related to access to healthcare, particularly in the areas of sexual and reproductive health (SRH), mental health and psychosocial support (MHPSS), and gender-based violence (GBV) response. However, the nature and intensity of these challenges varied significantly depending on the context. While settlement areas such as Kyaka II and Adjumani faced structural and capacity-related constraints, the urban context of Kampala was more influenced by socio-economic barriers and issues of integration.
Objectives of the evaluation
General Objective
The overall objective of this evaluation was to assess the relevance, adequacy, efficiency, effectiveness, impact, sustainability, and participatory nature of the project “Protecting the dignity of refugees in Uganda: responding to sexual and gender-based violence as a human rights violation and public health issue.” The evaluation aimed to generate evidence-based conclusions and practical recommendations to strengthen accountability, support organizational learning, and inform the design of future interventions targeting refugee populations in Uganda.
Specific Objectives
The evaluation specifically sought to:
Assess the extent to which the project achieved its planned results (R1–R4) and its Specific Objective, particularly in improving access to sexual and reproductive health (SRHR), mental health and psychosocial support (MHPSS), and gender-based violence (GBV) response services across Kampala, Kyaka II, and Adjumani.
Analyse the relevance and coherence of the project design in relation to the needs and priorities of refugee and host populations, as well as its alignment with national policies and humanitarian frameworks.
Examine the efficiency of the intervention in terms of the use of financial, human, and institutional resources, including the extent to which activities were implemented within planned timelines.
Evaluate the effectiveness and quality of implementation processes, including coordination mechanisms between Farmamundi, AHA, Emesco, and institutional stakeholders.
Assess the broader impact of the intervention on individuals, communities, and institutions, including both intended and unintended effects.
Determine the sustainability of project outcomes, including the extent to which benefits are likely to continue beyond the project period.
Analyse the level of participation, ownership, and accountability among rights-holders and local institutions, including the effectiveness of feedback and community engagement mechanisms.
Assess the integration of cross-cutting approaches, including gender and age sensitivity, human rights-based approaches, conflict sensitivity, and the principle of Do No Harm.
Purpose of the Evaluation
The evaluation served both a learning and accountability function. It aimed to provide a structured assessment of the project’s performance against its objectives and expected results, while also generating actionable insights to improve future programming.
Specifically, the evaluation was intended to:
Support implementing partners (Farmamundi, AHA, and Emesco) in identifying strengths, gaps, and lessons learned to enhance the quality, effectiveness and impact of future interventions.
Ensure accountability to donors, particularly the Basque Government, by demonstrating the extent to which resources were used effectively and results achieved.
Inform strategic decision-making by providing evidence on what worked, what did not, and why, within the different operational contexts of Kampala, Kyaka II, and Adjumani.
Contribute to broader learning within the humanitarian and development sector, particularly in relation to integrated approaches to health, protection, and gender-based violence in refugee settings.