06
RESULTS
This section presents the findings of the final external evaluation of the project “Protecting the dignity of refugees in Uganda: responding to sexual and gender-based violence as a human rights violation and public health issue.” The analysis examines the extent to which the intervention achieved its intended objective and results across the three implementation areas of Kampala, Kyaka II, and Adjumani. The findings are organized around the OECD-DAC evaluation criteria and complementary humanitarian criteria, namely relevance, effectiveness, efficiency, impact, sustainability, connectivity, coordination, coverage, ownership and participation, and cross-cutting issues. Particular attention is given to the project’s three core thematic pillars: access to essential health services, mental health and psychosocial support (MHPSS), and prevention and response to sexual and gender-based violence (SGBV).
The results are informed by a review of project documentation, the final project report, the logical framework, baseline and endline data sets, routine health and project monitoring data, and qualitative insights from stakeholder consultations. The analysis considers both the achievement of planned outputs and the broader contribution of the intervention to improved service access, strengthened community systems, enhanced survivor support, and accountability to affected populations. Given the diversity of the three implementation contexts, the findings also examine differences between the urban refugee setting of Kampala and the settlement-based contexts of Kyaka II and Adjumani, highlighting how the intervention responded to distinct operational realities, population needs, and service delivery challenges.
The evaluation adopted a mixed-methods approach that combined quantitative and qualitative evidence to examine both the measurable achievements of the project and the experiences and perceptions of the targeted populations and stakeholders. In line with the evaluation framework, the analysis draws from four principal layers of evidence: project implementation and monitoring data, comparative baseline and endline findings, qualitative evidence from Key Informant Interviews (KIIs) and Focus Group Discussions (FGDs), and the interpretation of the assessment team guided by the OECD-DAC and humanitarian evaluation criteria.
The first layer of evidence consisted of project documentation and routine implementation records, including the final project report, activity reports, monitoring data, DHIS2 records, training records, referral data, and accountability documentation. These sources provided evidence on the extent to which planned activities and outputs were achieved, including healthcare service delivery, deployment of outreach services, SGBV prevention and response interventions, psychosocial support services, awareness campaigns, and accountability mechanisms. This evidence was particularly important in assessing operational performance, implementation coverage, and progress against the logical framework indicators and expected results (R1–R4).
The second layer of evidence was derived from the comparative analysis of baseline and endline findings, which served as the principal quantitative basis for assessing changes associated with the intervention. The endline dataset was utilized as the household-level evidence base for the evaluation due to its methodological adequacy, broad thematic coverage, and direct alignment with the project indicators and evaluation questions. Comparative analysis between baseline and endline findings enabled the evaluation to assess trends and changes in areas such as access to healthcare services, awareness of sexual and reproductive health rights, community perceptions regarding SGBV services, participation in awareness activities, and utilization of accountability mechanisms. This approach also strengthened the evaluation’s ability to assess outcomes and emerging impacts beyond routine output monitoring.
The third layer of evidence was generated through KIIs and FGDs conducted with a broad range of stakeholders, including implementing partners, government representatives, healthcare workers, community leaders, Village Health Teams (VHTs), refugee structures, women, adolescents, and survivors accessing services. These consultations provided deeper insights into the lived experiences of beneficiaries and the operational realities of implementation across Kampala, Kyaka II, and Adjumani. Qualitative evidence helped contextualize quantitative findings by exploring perceptions of service quality, barriers to access, institutional coordination, community ownership, effectiveness of SGBV response mechanisms, and the perceived sustainability of project interventions. The KIIs and FGDs also provided important evidence regarding differences across implementation locations and population groups.
The final layer of evidence involved interpretation and judgement by the assessment team. Findings from different data sources were triangulated and analyzed against the project’s theory of change, logical framework, and evaluation criteria to determine not only whether activities were implemented, but also the extent to which they contributed to meaningful change within the refugee and host communities. This analytical approach enabled the evaluation to move beyond descriptive reporting and provide a deeper assessment of the project’s relevance, effectiveness, efficiency, impact, sustainability, coherence, and overall contribution to strengthening health systems and protecting the dignity of refugees in Uganda.
Achivement of the Objectives.
The project substantially contributed to the promotion of the right to health and the right to live with dignity among refugee populations in Kampala, Kyaka II, and Adjumani through a holistic intervention model that integrated primary healthcare, sexual and reproductive health (SRH), mental health and psychosocial support (MHPSS), gender-based violence (GBV) prevention and response, community engagement, and accountability mechanisms. Rather than approaching healthcare and GBV as isolated thematic areas, the intervention recognized the strong interrelationship between health inequities, displacement-related vulnerabilities, gender inequality, psychosocial distress, and barriers to accessing protection and justice. This integrated approach enabled the project to respond simultaneously to immediate humanitarian needs while also strengthening community-level systems, referral pathways, institutional coordination, and rights-based approaches to care.
Evidence from implementation reports indicates that the intervention improved access to essential healthcare services, expanded community awareness regarding health and rights, strengthened referral and support systems for survivors of sexual and gender-based violence, and increased the availability of mental health and psychosocial support services across the three operational contexts. The intervention also strengthened community participation and accountability structures, enabling refugee communities to play a more active role in identifying needs, shaping interventions, and providing feedback on services delivered. Importantly, the project addressed GBV innovatively through a secondary pathway of managing the medical consequences of violence and displacement, as well as the structural and social factors that increase vulnerability, including stigma, lack of information, weak referral pathways, social isolation, and limited community-level protection mechanisms.
At a broader level, the project demonstrated alignment with humanitarian protection principles, human rights approaches, and the localisation agenda by working through existing public systems, refugee-led structures, local authorities, Village Health Teams (VHTs), community committees, and local implementing partners. The intervention therefore contributed not only to service delivery outcomes but also to strengthening local ownership, institutional coordination, and community resilience. It is noteworthy that important structural challenges remained, including medicine stockouts, persistent stigma surrounding mental health and GBV, transportation barriers, and limitations within the broader health system. However, the overall implementation significantly advanced access to dignified, integrated, and survivor-centered services for refugee populations in the three intervention areas.
The specific objective of improving the health and sexual and reproductive health status of Congolese, South Sudanese, Somali, and other refugee populations through addressing sexual and gender-based violence as both a human rights violation and a public health issue was largely achieved. In relation to I.O.V.1.O.E, the intervention successfully expanded access to integrated health services with a strong focus on SRH, mental health, psychosocial support, GBV prevention and response, and community-based protection systems. Through the combined use of fixed health services, mobile outreach teams, referrals to specialized care, community sensitization, psychosocial support interventions, and survivor-centered legal and psychological assistance, the project addressed critical barriers that had previously limited access to comprehensive care among refugee communities.
In relation to I.O.V.2.O.E and I.O.V.3.O.E, The intervention also strengthened the capacities of healthcare workers, community leaders, and community structures to identify, prevent, refer, and respond to cases of GBV and other protection concerns. The dissemination of referral protocols, strengthening of community committees, establishment of accountability and feedback systems, and reinforcement of coordination between health, protection, and community actors contributed to a more structured and comprehensive response framework. In parallel, awareness-raising activities improved knowledge among refugee communities regarding available services, referral pathways, rights, gender equality, and prevention of violence, thereby supporting earlier care-seeking behavior and greater utilization of services.
Importantly, the project demonstrated adaptability to the differing realities of urban and settlement contexts. In Kyaka II and Adjumani, interventions largely focused on improving access to essential healthcare, infectious disease prevention, outreach services, and community-based systems in geographically dispersed settlements. In Kampala, the intervention increasingly responded to the growing burden of chronic illnesses, psychosocial distress, mental health conditions, and complex GBV cases affecting urban refugee populations. This contextual adaptation enhanced the intervention's relevance and improved responsiveness to the specific vulnerabilities in each operational area. Furthermore, in line with I.O.V.4.O.E, the intervention strengthened participation, accountability, and coordination mechanisms through community committees, dialogue platforms, feedback systems, and interagency coordination structures, contributing to more transparent, participatory, and community-centred humanitarian assistance.
The intervention demonstrated contextual adaptation across the three operational areas, responding to the distinct health, protection, and psychosocial realities affecting refugee populations in Kampala, Kyaka II, and Adjumani. In Kampala, the project increasingly addressed the complex challenges facing urban refugees, including fragmented access to healthcare, high out-of-pocket costs, chronic illnesses, psychosocial distress, mental health conditions, and protection concerns linked to poverty, social isolation, and insecure living conditions. In Kyaka II, the intervention focused more on improving access to essential healthcare, maternal and child health services, infectious disease prevention, and community-based outreach systems within a geographically dispersed settlement environment where distance and limited service coverage remained major barriers. In Adjumani, the project responded to vulnerabilities associated with remote settlement contexts, recurrent outbreak risks, weak access to specialized services, and high psychosocial needs among displaced populations, while simultaneously strengthening community-level awareness, referral, and protection mechanisms. This differentiated approach significantly enhanced the intervention's relevance and appropriateness across the three locations.
A major strength of the intervention was its layered implementation model, which linked community structures, outreach services, healthcare facilities, referral systems, psychosocial services, and institutional coordination mechanisms. This created multiple entry points through which refugees could access support, while simultaneously strengthening prevention, awareness, early identification, referrals, and continuity of care. The intervention also demonstrated strong alignment with national systems and humanitarian coordination mechanisms, reinforcing sustainability and local ownership.
Another major strength of the intervention was its ability to combine a unified strategic vision with flexible, context-sensitive implementation approaches across diverse humanitarian settings. While the project maintained a consistent focus on integrated healthcare, SRH, mental health, GBV prevention and response, accountability, and community participation, the operational emphasis evolved according to the realities of each location. Settlement-based interventions in Kyaka II and Adjumani relied heavily on mobile outreach systems, community structures, awareness activities, and referral coordination to address barriers linked to geography, infrastructure, and limited service availability. In contrast, interventions in Kampala increasingly focused on navigating fragmented urban systems, strengthening referrals, addressing chronic and mental health conditions, and responding to more complex social and protection vulnerabilities affecting urban refugees. This adaptability enhanced the overall effectiveness of the project and reinforced its alignment with rights-based, survivor-centered, and community-driven humanitarian programming principles.
The project further distinguished itself through its emphasis on participation and accountability. Refugee communities were not treated merely as beneficiaries, but increasingly as active participants through community committees, dialogue sessions, monitoring structures, VHT networks, and accountability mechanisms. This participatory approach strengthened trust, community acceptance, and responsiveness to emerging needs while contributing to greater transparency and inclusion.
Despite the strengths mentioned above, persistent systemic limitations continued to affect refugee access to healthcare and protection services, including shortages of supplies, high service demand, economic vulnerabilities, stigma, and weaknesses within broader referral systems. Regardless, the available evidence indicates that the intervention made a significant contribution to improving access to integrated healthcare and strengthening protection and support mechanisms for refugee populations across the three project locations.
Across the three operational areas, the intervention generated important foundations for longer-term improvements in health access, GBV prevention and response, mental health support, and community resilience. Although structural constraints within the humanitarian and public health environment remain significant, the project established stronger community and institutional systems that can support more coordinated, inclusive, and rights-based responses for refugee populations in Uganda. Overall, the project achieved strategic relevance and coherence by integrating healthcare delivery, protection, psychosocial support, community engagement, accountability, and institutional strengthening into a single, cohesive framework. The intervention moved beyond a narrow service-delivery approach to addressing interconnected drivers of vulnerability affecting refugee populations, particularly women, children, adolescents, and survivors of sexual and gender-based violence.
Achievement of intended outcomes and results
Outcome 1: Increased coverage, accessibility, and quality of essential healthcare among the refugee population in Kampala, Kyaka II, and Adjumani, with a focus on mental health and sexual and reproductive health, ensuring safe and appropriate care for survivors of sexual and gender-based violence.
Overall, Outcome 1 was achieved to a high degree across the three intervention areas. The intervention significantly expanded access to essential healthcare, sexual and reproductive health services, mental health and psychosocial support services, referral care, and community outreach services for refugee populations in Kampala, Kyaka II, and Adjumani. Most indicators under this outcome either met or substantially exceeded their planned targets, demonstrating strong implementation performance and the ability of the intervention to respond to diverse humanitarian and public health needs across both urban and settlement settings.
The achievement of Outcome 1 was driven through a combination of facility-based healthcare support, provision of medicines and medical supplies, deployment of integrated mobile outreach teams, referral coordination systems, mental health and psychosocial support interventions, healthcare worker training, and strengthened referral and coordination mechanisms. The intervention also demonstrated contextual adaptation across operational areas. In Kyaka II and Adjumani, interventions largely focused on improving access to essential healthcare, infectious disease prevention, maternal and child health services, and settlement-based outreach systems. In Kampala, the intervention increasingly responded to the growing burden of chronic illnesses, psychosocial distress, mental health conditions, orthopedic conditions, and complex referral needs affecting urban refugee populations.
Activity 1.1. Provision of essential medicines and medical supplies tailored to the needs of the refugee population, primarily for the reduction of maternal and child mortality and clinical care for SRH and sexual violence
This activity contributed significantly to improving the accessibility, coverage, and quality of healthcare services among refugee populations through the strengthening of health facility capacity and reduction of medicine stock-outs across the three operational locations.
The intervention began with joint assessments conducted alongside Kampala Capital City Authority (KCCA) and the District Health Offices in Kyegegwa and Adjumani to identify the most prevalent diseases, priority healthcare gaps, and recurrent medicine stock-outs affecting refugee-serving health facilities. The assessments incorporated a gender-sensitive and survivor-centered approach, with specific attention to maternal health, SRH, mental health, and care for survivors of sexual and gender-based violence. Procurement processes were conducted through competitive supplier selection procedures in accordance with procurement guidelines. Medicines and medical supplies were procured through approved suppliers including Henber Pharmacy, Tavos, Ronjo Diagnostics LTD, Pharmacy Company Limited, and Abacus Pharma Africa LTD. Distribution systems were aligned with OPM, OCHA, and UNFPA guidance, while stock management and accountability systems were reinforced within supported health facilities.
Linked Indicator: I.O.V.1.R.1.
Target 1: At least 10,600 refugees (6,500 in Kyaka II, 3,000 in Kampala, and 1,100 in Adjumani) receive medical care and medications at health centers.
Achievement: A total of 23,596 refugees received medical care and medications through supported health facilities, including 8,505 refugees in Kyaka II, 3,219 in Kampala, and 11,872 in Adjumani.
The intervention substantially exceeded its original healthcare coverage target. In Kyaka II and Adjumani, medicines primarily supported treatment of malaria, pneumonia, diarrhea, maternal and child health conditions, and infectious disease outbreaks, while also strengthening SRH and HIV-related services. In Kampala, medicine procurement increasingly responded to chronic illnesses, orthopedic conditions, and mental health-related healthcare needs among urban refugee populations.
The activity also strengthened preparedness and response capacities during public health threats including Ebola, Mpox, and Crimean-Congo Hemorrhagic Fever outbreaks through provision of sanitation materials, infection prevention supplies, and diagnostic commodities.
The intervention contributed to reducing healthcare access barriers associated with medicine stock-outs, particularly among vulnerable populations such as women, children under five, survivors of GBV, and individuals requiring chronic care support.
Baseline/Endline Changes
 The household surveys
captured tangible shifts in healthcare-seeking patterns and perceptions
of medicine availability between the baseline (n=815: Kyaka II 310,
Kampala 253, Adjumani 252) and endline (n=796: Kyaka II 327, Kampala
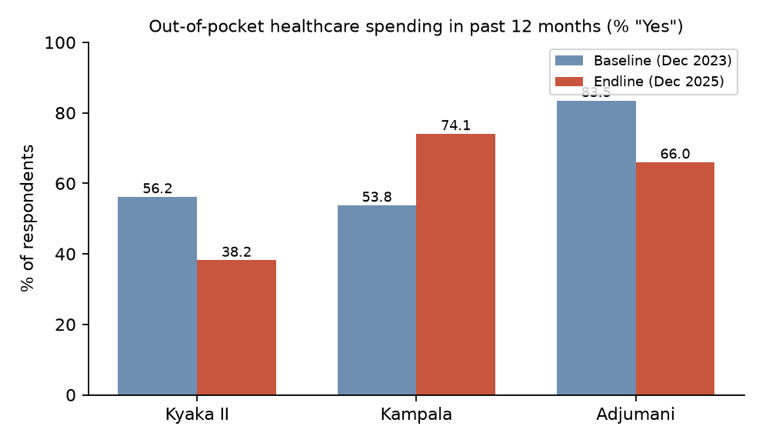
271, Adjumani 198). Reported out-of-pocket spending on healthcare in the
past 12 months fell substantially in two of the three sites — from 56.2%
to 38.2% in Kyaka II and from 83.5% to 66.0% in Adjumani — consistent
with the project's contribution to reducing stock-outs at supported
facilities. In Kampala, however, the proportion reporting healthcare
expenditure rose from 53.8% to 73.6%, reflecting the more privatised,
chronic-care orientation of urban refugee healthcare needs, toward which
the project's procurement was increasingly redirected. The proportion of
respondents who actually received treatment when they sought care at a
Government Health Centre or VHT increased in Kyaka II (94.4%→98.9%) and
especially in Kampala (87.3%→100.0%), indicating improved on-the-spot
availability of medicines and supplies at supported entry points.
Perceived availability of medicines (5-point scale) was broadly stable
in Kyaka II (3.10→3.14) but declined in Kampala (3.65→2.80) and Adjumani
(3.22→2.94), reflecting growing demand and remaining gaps despite
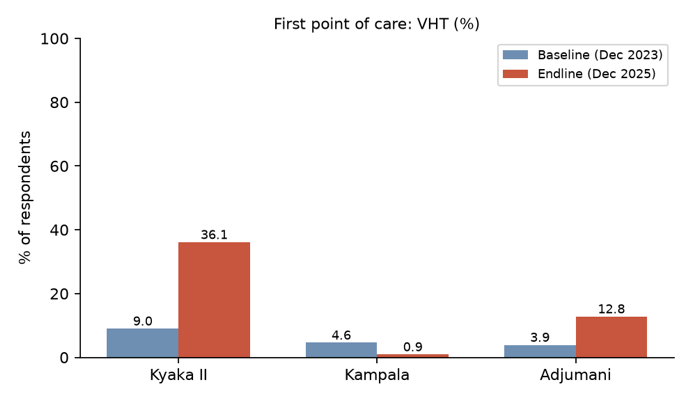
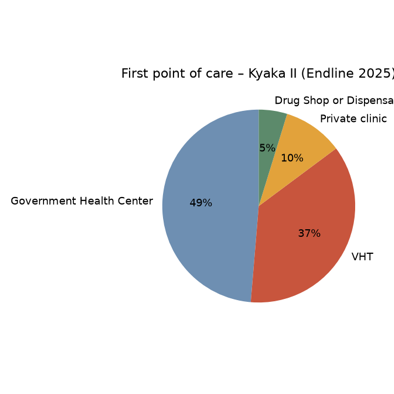
project inputs. The share who first turned to a Government Health Centre
when sick declined in all three sites — most notably in Kyaka II
(80.4%→48.2%) — with a corresponding rise in first-contact use of VHTs
(Kyaka II 9.0%→36.1%; Adjumani 3.9%→12.8%), indicating successful
task-shifting toward community-based service points strengthened by the
project.
The household surveys
captured tangible shifts in healthcare-seeking patterns and perceptions
of medicine availability between the baseline (n=815: Kyaka II 310,
Kampala 253, Adjumani 252) and endline (n=796: Kyaka II 327, Kampala
271, Adjumani 198). Reported out-of-pocket spending on healthcare in the
past 12 months fell substantially in two of the three sites — from 56.2%
to 38.2% in Kyaka II and from 83.5% to 66.0% in Adjumani — consistent
with the project's contribution to reducing stock-outs at supported
facilities. In Kampala, however, the proportion reporting healthcare
expenditure rose from 53.8% to 73.6%, reflecting the more privatised,
chronic-care orientation of urban refugee healthcare needs, toward which
the project's procurement was increasingly redirected. The proportion of
respondents who actually received treatment when they sought care at a
Government Health Centre or VHT increased in Kyaka II (94.4%→98.9%) and
especially in Kampala (87.3%→100.0%), indicating improved on-the-spot
availability of medicines and supplies at supported entry points.
Perceived availability of medicines (5-point scale) was broadly stable
in Kyaka II (3.10→3.14) but declined in Kampala (3.65→2.80) and Adjumani
(3.22→2.94), reflecting growing demand and remaining gaps despite
project inputs. The share who first turned to a Government Health Centre
when sick declined in all three sites — most notably in Kyaka II
(80.4%→48.2%) — with a corresponding rise in first-contact use of VHTs
(Kyaka II 9.0%→36.1%; Adjumani 3.9%→12.8%), indicating successful
task-shifting toward community-based service points strengthened by the
project.
KII/FGD Perspectives
Alleviating Immediate Supply Shortfalls The
qualitative evidence robustly substantiates the quantitative finding
that the project successfully mitigated out-of-pocket health
expenditures, specifically within settlement settings. Both healthcare
providers and community members indicated that prior to the
intervention's supply buffers, frequent stock-outs forced refugees to
independently purchase essential drugs. However, the direct supply of
commodities by implementing partners (AHA and EMESCO) established vital
safety nets. As one psychiatric nurse observed, "These medicines,
like things like PrEP... are required for managing the cases. And once
you have out of stock... it affects the case" (KII, Psychiatric
Nurse, AHA). By filling these gaps, the project  preserved healthcare access for
the most vulnerable.
preserved healthcare access for
the most vulnerable.
 Urban vs Settlement
Disparities in Care Seeking. Conversely, Kampala saw an
increase in out-of-pocket expenditure, a reality qualitative insights
attribute to the complex, chronic-care nature of urban healthcare
demands compared to the primary-care focus in settlements. Urban
patients frequently presented with non-communicable diseases requiring
specialised, costly medications that the project's essential drug supply
could not always cover. An urban respondent highlighted the frustration
of receiving generic analgesics for specific maladies: "Maybe you're
having headache. They give you something that can help on that, but they
don't give you the specific drug you have to take" (FGD, Men,
Kampala). Similarly, a settlement commandant verified this
limitation, noting that the project provided "essential drugs... but
how about other drugs for complicated sicknesses?" (KII,
Settlement Commandant, OPM, Adjumani). Consequently, the capacity
of VHTs as first-responders effectively absorbed routine primary care
needs within communities, but urban refugees requiring advanced
morbidities management still faced considerable financial burdens.
Urban vs Settlement
Disparities in Care Seeking. Conversely, Kampala saw an
increase in out-of-pocket expenditure, a reality qualitative insights
attribute to the complex, chronic-care nature of urban healthcare
demands compared to the primary-care focus in settlements. Urban
patients frequently presented with non-communicable diseases requiring
specialised, costly medications that the project's essential drug supply
could not always cover. An urban respondent highlighted the frustration
of receiving generic analgesics for specific maladies: "Maybe you're
having headache. They give you something that can help on that, but they
don't give you the specific drug you have to take" (FGD, Men,
Kampala). Similarly, a settlement commandant verified this
limitation, noting that the project provided "essential drugs... but
how about other drugs for complicated sicknesses?" (KII,
Settlement Commandant, OPM, Adjumani). Consequently, the capacity
of VHTs as first-responders effectively absorbed routine primary care
needs within communities, but urban refugees requiring advanced
morbidities management still faced considerable financial burdens.
Activity 1.2. Provision of safe medical testing at national hospitals in Kampala for refugees referred from the Kyaka II, Kampala, and Adjumani settlements
This activity strengthened access to specialized diagnostic services and referral healthcare for refugees requiring advanced medical investigations and treatment beyond the capacity of settlement-based and lower-level health facilities.
The intervention established structured referral coordination systems involving referral screening, appointment scheduling, transportation support, accommodation through medical shelters, follow-up coordination, and linkages with national referral hospitals and specialized diagnostic facilities in Kampala. Emergency and mental health cases were prioritized through rapid referral systems, while elective referrals were managed through scheduled coordination mechanisms involving settlement partners and referral coordinators. The intervention also supported transportation, accommodation, and continuity of care for patients requiring prolonged follow-up and specialist review services. Referral systems were strengthened through coordination between AHA, settlement partners, referral hospitals, AIRD, and specialized laboratories.
Linked Indicator: I.O.V.2.R.1.
Target: At least 1,500 refugees referred for safe medical testing, analysis, and diagnosis at national referral hospitals in Kampala.
Achievement: A total of 1,780 refugees received referral support for specialized medical testing and diagnosis, of whom approximately 59% were women and children under five.
The project exceeded the planned referral target and significantly strengthened access to specialized healthcare for refugees across Uganda. While referrals originated from Kyaka II, Kampala, and Adjumani, the intervention also supported refugees from other settlements, including Rwamwanja, Palorinya, Kyangwali, and Nakivale. The largest proportion of referral cases involved cancer-related conditions (468 cases), musculoskeletal disorders (393 cases), cardiovascular conditions (203 cases), neurological disorders (142 cases), nephrology and urological conditions (104 cases), and gastrointestinal conditions (99 cases). These findings highlighted the growing burden of chronic illnesses, complex medical conditions, and specialized healthcare needs among refugee populations.
Geographical variations were evident across operational areas. In settlement contexts such as Kyaka II and Adjumani, referrals were frequently linked to limited specialist availability and gaps in diagnostic capacity at local health facilities. In Kampala, referral systems increasingly responded to complex urban refugee healthcare needs, including chronic diseases, orthopedic injuries, mental health conditions, and advanced diagnostic requirements. The activity also contributed to improved efficiency within the referral system through strengthened verification mechanisms, increased use of lower-level facilities where appropriate, and the introduction of reverse referral approaches involving specialist outreach to settlements.
Baseline/Endline Changes
Endline data show measurable progress in access to clinicians, particularly in Adjumani where the proportion of respondents reporting difficulties accessing a doctor or clinical professional in the past 12 months fell from 42.7% to 30.9%. In Kyaka II and Kampala the indicator remained essentially flat (34.3%→39.3% and 42.3%→44.7% respectively), consistent with persistent specialist gaps that the referral pathway is designed to address rather than eliminate at local level. Mean ratings for inpatient services, triage and ambulance services were collected on Likert scales in both rounds, but the most actionable shift is the strong endline endorsement of referral-style support: when combined with the project's monitoring data on 1,780 specialised referrals (target 1,500), the survey evidence supports the conclusion that referral support partially compensated for unresolved specialist shortages at the primary level, especially in Adjumani.
KII/FGD Perspectives
Bridging Diagnostic Gaps Through Coordination The establishment of a structured referral mechanism addressed a critical void in refugee health infrastructure. Stakeholders noted that prior to the intervention, refugees requiring advanced diagnostics, surgeries, or cancer care faced immense logistical and financial barriers. The project’s facilitation of safe transport, accommodation, and procedural appointments at national facilities directly contributed to the overachievement of referral targets. A medical hostel run by AHA was frequently cited as a crucial halfway point for rural refugees undertaking treatment in Kampala. One community member recalled, "They were in Kampala for four months. They were being taken care of by AHA and they were in Mulago Hospital" (FGD, Women Survivors, Kyaka II).
Persisting Urban Navigation and Systems Challenges: Despite marked improvements, qualitative accounts reveal that tracking and closing the referral loop remain significant hurdles. Incomplete paperwork and staffing rotations at receiving hospitals frequently disrupted the feedback cascade required for comprehensive case management. Furthermore, recent funding constraints have threatened the sustainability of urban referral coordination, leaving local health workers struggling. A clinical officer lamented the breakdown of the pathway, stating, "Right now, the referral pathway is quite a big issue... we don't have a support system that is helping us" (KII, Clinical Officer, MTI, Kyaka II). Thus, while the intervention effectively bypassed local specialist deficits momentarily, long-term sustainability demands deeper institutional embedding.
Activity 1.3. Training of health personnel in the prevention of communicable diseases and in maternal-child and SRH care, ensuring safe and appropriate care for survivors of sexual and gender-based violence (including mental health)
This activity aimed to strengthen the technical capacity of healthcare workers to provide quality, gender-sensitive, rights-based, and culturally appropriate healthcare services for refugee populations across the three operational areas.
Training activities targeted healthcare workers from public health facilities, refugee-serving private facilities, referral centers, and community health systems. The trainings addressed maternal and child health, infectious disease prevention, mental health management, SRH services, GBV case management, prenatal and postnatal care, breast and cervical cancer screening, survivor-centered response, and referral coordination systems.
Participatory methodologies including simulations, case studies, discussions, group work, role plays, and practical demonstrations were used to strengthen both technical competencies and applied clinical skills.
Linked Indicator: I.O.V.3.R.1.
Target 1: 75% of 60 healthcare professionals participate in specialized training courses and apply the knowledge acquired.
Achievement: A total of 241 healthcare professionals participated in specialized training activities, with post-training assessments demonstrating significant improvement in technical knowledge and competencies. (average post-test score all increased)
The intervention substantially exceeded its original healthcare worker training target. Training coverage expanded far beyond initial projections due to high demand and identified capacity gaps across health facilities serving refugee populations.
In Kampala, trainings focused strongly on urban refugee healthcare challenges, including prenatal and postnatal care, family planning, cancer screening, GBV case management, and survivor-centered care approaches. In Kyaka II, the focus was more strongly linked to infectious disease prevention, maternal-child health, and settlement-specific healthcare challenges. In Adjumani, trainings emphasized epidemic preparedness, infection prevention and control, mental health screening, and clinical management of GBV cases, including coordination with police and protection actors.
Pre- and post-training assessments consistently demonstrated strong improvements in technical knowledge across all training themes and operational areas. The trainings also strengthened coordination between healthcare providers, protection actors, police, referral systems, and community structures.
Despite these achievements, high staff turnover within health facilities remained a significant challenge affecting continuity of institutional capacity. Participants also identified the need for ongoing refresher training, mentorship, and increased availability of clinical tools, referral materials, and medical supplies.
Baseline/Endline Changes
Community-level perceptions of provider behaviour — a proxy for the quality dimensions targeted by the training package — showed mixed but generally positive movement. The frequency with which providers reportedly asked for patients' opinions/beliefs about their care improved in Kyaka II (mean 2.84→3.28 on a 5-point scale) and Kampala (3.27→3.48), while remaining stable in Adjumani (3.22→3.19). Use of interpreters to understand patients' healthcare needs improved in Kampala (85.5%→94.0%) but declined in Kyaka II (76.8%→54.1%) and Adjumani (91.5%→85.6%), pointing to language-mediation gaps that persist despite training. Likert-scale ratings of counselling, family planning, maternal and VHT services were generally above 3.5/5 at endline in Kampala and Adjumani, with Kyaka II somewhat lower — consistent with the training emphasis (urban GBV management/cancer screening in Kampala; epidemic preparedness and GBV clinical management in Adjumani) and underscoring continued exposure of newly-deployed staff in Kyaka II to staff turnover-related quality dips.
KII/FGD Perspectives
Enhanced Clinical Confidence and Competence The qualitative data aligns with the reported knowledge improvements following the specialised training initiatives. Health personnel and implementing partners highlighted that the capacity building empowered staff to confidently manage sensitive issues, particularly clinical responses to GBV. Prior to the intervention, many facilities lacked the specialised personnel needed to conduct forensic examinations or administer immediate post-rape care. Following training, the number of capable responders surged noticeably. One GBV focal person recalled, "Before, we had about six health workers who were competently... but after last year's training, our number went up to about 12" (KII, GBV Officer MTI, Kyaka II).
Persistent Communication and Systems Barriers While clinical competencies improved, the survey’s mixed findings regarding provider behaviour are echoed in the transcript narratives. The application of survivor-centred care remains partially hindered by systemic deficits, primarily staff turnover and linguistic barriers. Respondents stressed that quality care hinges on clear communication, yet many facilities still grapple with interpreter shortages, leading to compromised patient experiences. "We need more interpreters... we have a shortage of them," admitted a psychiatric nurse (KII, Psychiatric Nurse, AHA). Similarly, high fatigue among the limited remaining staff occasionally resulted in adverse patient encounters, indicating that while training is efficacious, it is frequently offset by resource strain and language disconnects.
Activity 1.4. Dissemination of the healthcare protocol and standard operating procedures among healthcare personnel from the perspective of integrating the components of acceptability, gender, and human rights into clinical practice
This activity strengthened understanding and implementation of referral standard operating procedures (SOPs) and coordination mechanisms among health, protection, and referral actors across Kampala, Kyaka II, and Adjumani.
The intervention responded to increasing pressure on referral systems caused by inappropriate referrals, limited understanding of referral criteria, weak coordination, and growing demand for specialized services. Participatory dissemination and coordination meetings were conducted involving healthcare workers, district authorities, UNHCR, OPM, referral hospitals, and implementing partners.
Linked Indicator: I.O.V.3.R.1.
Target: Dissemination of one protocol for action among healthcare staff.
Achievement: One referral protocol and associated standard operating procedures were disseminated and operationalized among healthcare stakeholders across the three operational areas.
A total of 42 stakeholders participated in dissemination sessions in Kampala, 44 in Kyaka II, and 20 in Adjumani. The activity strengthened shared understanding regarding referral criteria, documentation requirements, coordination responsibilities, and survivor-centered referral pathways.
The intervention also facilitated identification of key referral bottlenecks including shortages of specialists, transportation barriers, supply limitations, and weaknesses in health information systems. Discussions generated recommendations to strengthen referral coordination, improve prioritization processes, and reinforce monitoring systems.
The activity contributed to improving coordination, standardization, accountability, and efficiency within refugee referral systems while reinforcing principles of dignity, gender sensitivity, human rights, and equitable healthcare access.
Baseline/Endline Changes
Awareness of protocol-related coordination practices was used as a community-level proxy for SOP dissemination. Reported agency engagement with community leadership on cultural appropriateness of services improved strongly in Kampala (73.8%→89.8%) but declined in Kyaka II (77.0%→53.1%) and Adjumani (87.4%→72.0%), suggesting that protocol dissemination translated more visibly into urban coordination structures than settlement-level routine practice. Reported attendance at post-distribution meetings about medicines supplied to the community declined across all sites (Kyaka II 56.2%→44.6%; Kampala 57.8%→22.7%; Adjumani 67.5%→63.5%), indicating that, although the referral SOP was operationalised among 106 stakeholders across the three sites, downstream community feedback loops on supply chains weakened — a gap the evaluation flags for the sustainability plan.
KII/FGD Perspectives
Strengthened Inter-Agency Synergy The dissemination of standard operating procedures (SOPs) successfully fostered improved coherence among stakeholders. KIIs across all sites confirmed that grounding healthcare, legal, and psychosocial services within integrated protocols fundamentally enhanced service delivery. Implementing partners indicated that formalised coordination meetings dismantled previous silos, facilitating smoother intra-agency referrals. By aligning on survivor-centred protocols, local organisations established a clearer chain of custody for GBV cases. "At the end of it all, we are able to compile the information and also disseminate... for though maybe there was a complaint to your organization, there and then you get the question" (KII, GBV Officer MTI, Kyaka II).
Translating Policy into Community Practice However, while institutional coordination surged, translating these SOPs into tangible grassroots knowledge encountered obstacles. Community-level understanding of referral pathways, particularly regarding medical supply chains, appeared to wane, validating the survey's recorded decline in post-distribution accountability. Local leaders noted that while upper-level protocols were robust, downstream feedback mechanisms requiring community members to understand these SOPs were occasionally lacking. A public health officer stressed the need to contextualize protocol dissemination: "You have to collaborate with your partner, with the IP... and then, since we are operating partners now, you have to coordinate with the lead IP in health" (KII, Public Health Officer, EMESCO, Adjumani). Ultimately, while institutional harmonisation succeeded, deeper community integration of these protocols remains an ongoing requirement.
Activity 1.5. Coordination of mobile health teams to bring health and mental health services closer to the refugee population in the settlements of Kampala, Kyaka II, and Adjumani
This activity became one of the most important service delivery mechanisms under Outcome 1, significantly expanding healthcare access among geographically isolated, underserved, and highly vulnerable refugee populations.
The mobile outreach teams operated through close coordination with district authorities, health facilities, community leaders, VHTs, refugee structures, and partner organizations. The teams addressed major barriers related to distance, transportation costs, overcrowded facilities, health facility closures, linguistic barriers, and limited specialized services.
Linked Indicator: I.O.V.1.R.1.
Target 2: 19,200 people served by 240 deployed mobile health teams.
Achievement: A total of 24,115 people were reached through 243 integrated mobile health teams deployed across Kampala, Kyaka II, and Adjumani.
The intervention exceeded both outreach and coverage targets. In Kampala, 83 mobile outreach teams reached 7,615 individuals. In Kyaka II, 80 outreach teams reached 7,992 individuals, while in Adjumani, 80 outreach teams reached 8,508 individuals.
Services delivered included SRH services, antenatal care, immunization, STI screening, HIV testing, malaria testing, family planning, nutritional screening, health education, disease prevention, counseling, chronic disease management, and referrals for specialized services.
Geographical distinctions strongly shaped implementation priorities. In Kyaka II and Adjumani, outreach activities primarily addressed infectious disease prevention, maternal-child health, immunization, and settlement access barriers. In Kampala, the mobile teams increasingly responded to fragmented urban healthcare access systems, chronic illnesses, and growing psychosocial and mental health needs.
The outreach activities also strengthened community engagement, health promotion, disease prevention, and early case identification while reinforcing referral pathways and linkages between communities and healthcare systems.
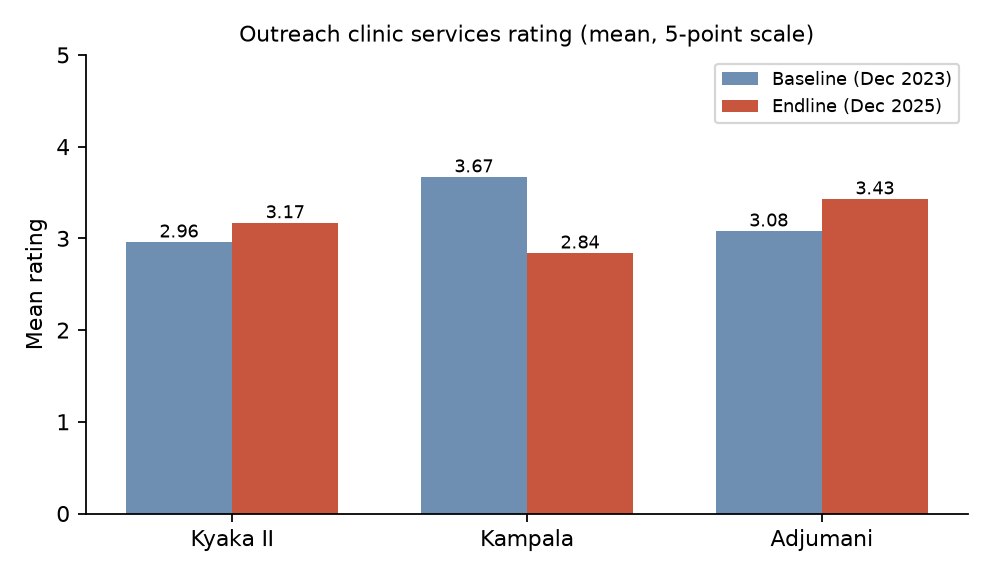
Baseline/Endline Changes
Community-level indicators of outreach exposure improved in Adjumani — VHT/health-worker education on diarrhoea prevention rose from 74.3% to 88.3%, and ratings of outreach clinics improved from 3.08 to 3.43 — confirming the strong settlement-level traction of the 80 mobile teams deployed there. In Kyaka II the headline outreach rating also improved (2.96→3.17), although malaria-prevention sensitisation reported by households fell (76.0%→57.8%), reflecting the dispersed geography of the settlement and shifting outreach priorities during outbreak responses. Kampala showed declining household-level rating of outreach (3.67→2.85) even though absolute coverage (7,615 people reached) was strong: this is consistent with the more fragmented urban operating environment, where mobile teams reach individuals who are less likely to recognise outreach as a structured service. Across the three sites, the 24,115 people reached by 243 mobile teams clearly exceeded the 19,200/240 target.
KII/FGD Perspectives
Decentralising Care in Settlement Geographies The mobile health teams were overwhelmingly identified as a transformative success, particularly in geographically expansive settlements like Adjumani and Kyaka II. By deploying medical and psychosocial support directly to distant communities, the project bypassed major structural barriers, including transport costs and physical immobility. Transcripts reveal that community members highly valued these outreaches, frequently treating them as standalone health centres. "When we go, those communities take it as a health centre. So the turn up is very enormous" (KII, Public Health Officer, EMESCO, Adjumani). These brigades simultaneously lightened the burden on primary facilities, improving wait times and easing health-system congestion.
Navigating Urban Fragmentation Challenges. Conversely, deploying mobile teams within Kampala yielded high numerical reach but diluted community-level recognition, aligning with the survey's declining outreach ratings for the urban site. The dispersed nature of urban refugees complicates the visibility of structured interventions. However, the teams functionally served their purpose by identifying individuals unable to navigate the national health system. Health workers noted that while urban outreach is logistically challenging, it remains vital for capturing vulnerable sub-groups who miss formal facility care. "We have clusters whereby we know that maybe in Nsambya, we have so many Congolese... So we ensure we take services closer to them" (KII, MEAL Officer, AHA, Kampala). The strategy succeeded in volume but inherently struggled with public visibility in urban sprawl.
Activity 1.6. Psychological therapy sessions to address the mental health and psychosocial needs of the population in situations of prolonged displacement
This activity significantly strengthened access to mental health and psychosocial support services for refugee populations experiencing trauma, psychosocial distress, anxiety, depression, prolonged stress, and social isolation associated with displacement and humanitarian vulnerability.
The intervention utilized group interpersonal therapy, psychosocial support groups, counseling, psychoeducation, community follow-up, and referrals to specialized psychiatric services. Sessions emphasized trauma-informed care, dignity, confidentiality, resilience building, coping mechanisms, and strengthening of social support systems.
Linked Indicator: I.O.V.4.R.1.
Target 1: 320 people served through at least 60 psychosocial therapy sessions.
Achievement: A total of 1,129 people participated in 240 psychosocial therapy sessions across the three operational areas.
Linked Indicator: I.O.V.4.R.1.
Target 2: 1,800 refugees access SMAPS services through 240 mobile teams.
Achievement: A total of 6,279 refugees accessed mental health and psychosocial support services through 279 mobile mental health outreach teams.
The intervention substantially exceeded planned targets for both therapy participation and outreach coverage, reflecting the very high burden of unmet mental health and psychosocial support needs among refugee populations.
In Kampala, mental health activities increasingly focused on trauma, depression, anxiety, psychosocial distress, and severe mental health conditions among urban refugees. In Kyaka II and Adjumani, activities focused more strongly on psychosocial support, community-based screening, trauma recovery, psychoeducation, and strengthening coping mechanisms within settlement communities.
The intervention also strengthened referral systems for severe mental health conditions requiring specialized psychiatric care, including referrals to Butabika National Referral Hospital and enrollment into ongoing psychosocial support systems.
Despite significant achievements, barriers such as stigma, language differences, transportation challenges, economic vulnerability, and competing livelihood responsibilities continued to affect regular participation in some settings. Nevertheless, the intervention substantially improved access to mental health services, reduced stigma surrounding psychosocial support, strengthened community awareness, and reinforced continuity of care for vulnerable refugee populations.
Baseline/Endline Changes
MHPSS is the area in which the survey data show the strongest and most consistent improvement. The composite question on access to quality MHPSS through psychosocial therapy and mobile teams rose from 2.94 to 3.17 in Kyaka II, from 2.76 to 3.49 in Adjumani, and only marginally declined in Kampala (3.80→3.66, from an already high baseline). Ratings of mental health services improved from 3.24 to 4.14 in Adjumani and were essentially stable at high levels in Kyaka II (3.75→3.78) and Kampala (4.41→4.13). General "mental health support" ratings improved in Kyaka II (3.08→3.21) and Adjumani (2.87→3.34). Combined with the project's reach of 6,279 refugees through 279 mobile mental health teams and 1,129 participants in 240 therapy sessions (against targets of 1,800/240 teams and 320/60 sessions respectively), these gains substantiate one of the clearest demonstrable behavioural and perceptual changes attributable to the intervention.
KII/FGD Perspectives
De-stigmatising Mental Health Interventions The qualitative evidence underscores mental health and psychosocial support (MHPSS) as one of the intervention’s most profoundly appreciated success stories. MHPSS therapies introduced novel coping mechanisms to populations burdened by immense displacement trauma, severe economic distress, and compounding reductions in food rations. Stakeholders observed that group therapies (IPTG) provided communal solace, demonstrating to participants that they were not suffering in isolation. A psychiatric nurse reflected on this shift: "The one who thinks he’s the only one person to do it will get hope... 'Oh, I'm not alone'" (KII, Psychiatric Nurse, AHA). This communal solidarity effectively eroded long-standing cultural stigmas attached to mental distress.
Coping with Structural Displacement Stressors The extraordinary demand for SMAPS mobile teams correlates strongly with external shocks affecting the refugee population, particularly acute subsistence challenges. While the therapy sessions vastly improved emotional resilience, HCWs noted that physiological stability was frequently undermined by practical realities like food insecurity. Nevertheless, the therapies fundamentally shifted community mindsets from reactive despair to proactive resilience. "They were able to share... what others were going through and even some even came up with solutions on how to overcome some of these concerns" (KII, SRHR Officer, Makasi, Kampala). This community-level emotional fortification validates the steep rise in MHPSS access ratings logged during the endline surveys.
Outcome 2: Community capacities strengthened to reduce inequalities in access to and use of health resources, improve comprehensive care for refugee women who are survivors of sexual and gender-based violence, and promote a life free from violence.
Overall, Outcome 2 was achieved to a high degree across Kampala, Kyaka II, and Adjumani. The intervention significantly strengthened community-level prevention, awareness, referral, mediation, psychosocial support, and survivor assistance systems related to sexual and gender-based violence (SGBV), sexual and reproductive health (SRH), gender equality, and community health promotion. Most indicators under this outcome either achieved or exceeded their planned targets, demonstrating strong community engagement and expansion of localized protection and support systems within both settlement and urban refugee contexts.
The achievement of Outcome 2 was supported through integrated community mobilization approaches involving community leaders, Village Health Teams (VHTs), refugee-led structures, community committees, local leaders, and institutional actors. The intervention combined capacity strengthening, awareness-raising, survivor-centered psychosocial and legal support, community dialogue mechanisms, and distribution of dignity and hygiene materials to address both immediate vulnerabilities and structural barriers affecting refugee populations, particularly women and girls.
Activity 2.1. Training of community leaders in awareness-raising techniques to promote gender equality and mechanisms for the prevention, detection, and mitigation of sexual and gender-based violence
This activity strengthened the capacity of community leaders and community structures to serve as frontline actors in the prevention, identification, mediation, referral, and response to sexual and gender-based violence within refugee communities.
Training sessions were conducted across Kampala, Kyaka II, and Adjumani targeting community health workers, VHTs, GBV committee members, refugee leaders, and representatives of refugee-led organizations. The trainings focused on gender equality, human rights, survivor-centered response, referral pathways, awareness-raising techniques, conflict mediation, PSEA, community mobilization approaches, communication strategies, and prevention of violence against women and girls. Participatory methodologies, including simulations, discussions, group exercises, role plays, and case studies, were used to strengthen the practical application of knowledge within community settings.
Linked Indicator: I.O.V.1.R.2.
Target 1: At least 80% of 60 community leaders participating in training modules demonstrate knowledge on prevention, mediation, and referral of cases of violence against women and GBV.
Achievement: A total of 62 community leaders participated in training activities, of whom 57.5% were women, with post-training assessments demonstrating significant improvement in knowledge related to prevention, mediation, referral pathways, and survivor-centered approaches.
The intervention exceeded the planned target for community leader participation while strengthening localized community prevention and referral systems across the three operational areas.
In Adjumani, the training emphasized prevention of gender inequality, human rights violations, and alternative dispute resolution within settlement communities. In Kyaka II, the training strongly focused on awareness-raising methodologies, communication techniques, community campaigns, and the role of VHTs and local structures in GBV prevention and health promotion. In Kampala, the training adopted a more technical and inter-agency orientation emphasizing SASA! methodologies, PSEA, urban referral systems, and survivor-centered coordination within complex urban refugee settings.
Pre- and post-test assessments demonstrated substantial improvements in participant knowledge across all operational areas. Participants also positively rated the relevance and applicability of the training content within their community engagement roles.
The activity contributed to strengthening early identification and referral of GBV cases, improving community awareness, reinforcing local leadership capacities, and promoting gradual shifts in harmful social norms linked to gender inequality and violence.
Baseline/Endline Changes
The most striking baseline-to-endline shift across the entire dataset is the increase in reported participation in AHA/EMESCO awareness-raising and training activities in Adjumani — from 18.5% at baseline to 75.1% at endline (+56.6 pp). Kampala also recorded a sharp gain (62.2%→77.3%), while Kyaka II declined modestly (68.2%→58.5%). Community awareness of GBV-prevention programmes rose substantially in Kampala (46.3%→65.5%) and Adjumani (52.9%→66.8%) but fell in Kyaka II (63.6%→36.0%), consistent with high baseline saturation in Kyaka II combined with respondent rotation between rounds. Taken with the 62 community leaders trained (57.5% women) and the post-training knowledge gains documented in monitoring data, the survey evidence demonstrates substantial community-level diffusion of GBV-prevention knowledge, especially in Adjumani.
KII/FGD Perspectives
Empowering Frontline Local Leadership: The strategy of equipping community leaders, RWCs, and VHTs with comprehensive knowledge of GBV prevention and response yielded significant structural dividends. Qualitative data extensively confirms that anchoring these training modules within existing community hierarchies ensured cultural appropriateness and facilitated wider dissemination. In Adjumani, where engagement metrics surged, trained leaders became the primary conduits for conflict mediation and first-response crisis management. Transcripts reveal a grassroots appreciation for interventions that bestowed permanent proficiencies over temporary material aid. One survivor noted, "When somebody has given you a skill, it is more better than giving money... The little knowledge they have empowered us, we shall not forget" (FGD, Women Survivors, Adjumani).
Sustaining Knowledge Amid Volunteer Turnover: While knowledge acquisition was universally commended, sustaining these leadership structures proved challenging. In Kyaka II and Kampala, the dip in visible community awareness often correlated with volunteer fatigue and staff rotation. Implementing partners noted that despite intensive capacity-building, leaders operating without stipends or sustained logistical support struggled to continuously enact their training. "Before they were only depending to their men... [the training was] empowering them to be self-resilient" (FGD, VHTs, Kyaka II). Thus, while the training successfully shifted foundational attitudes towards gender equality and violence prevention, the long-term operational viability of these community leaders remains vulnerable to economic attrition.
Activity 2.2. Awareness-raising and advocacy actions to promote SRH, gender equality, and the prevention of violence
This activity became one of the largest community engagement components under Outcome 2, significantly expanding access to information on health rights, sexual and reproductive health, gender equality, GBV prevention, referral pathways, mental health, communicable disease prevention, and available support services.
Awareness-raising activities were implemented through community dialogues, group sensitization sessions, door-to-door outreach, public awareness campaigns, and engagement within churches, schools, water points, markets, community gatherings, and refugee settlements. Community leaders, VHTs, refugee committees, and community structures played central roles in mobilization and message dissemination.
Linked Indicator: I.O.V.2.R.2.
Target: 20,000 people reached through information sessions led by community leaders on health promotion, SRH, gender equality, and prevention and response services for survivors of SGBV.
Achievement: A total of 22,660 people were reached through awareness-raising and sensitization activities, including 12,183 people in Kyaka II, 5,657 people in Kampala, and 4,820 people in Adjumani.
The intervention exceeded its planned awareness-raising target and significantly strengthened community knowledge regarding health promotion, SRH, gender equality, mental health, communicable disease prevention, survivor rights, and referral systems.
In Adjumani, sensitization activities strongly emphasized communicable disease prevention, immunization, maternal and child health, outbreak preparedness, and GBV prevention within settlement settings. In Kyaka II, awareness sessions heavily focused on refugee rights, SRH, gender equality, prevention of violence, referral pathways, and disease prevention in geographically dispersed communities. In Kampala, activities increasingly addressed mental health, urban GBV risks, family planning, psychosocial distress, and access barriers affecting urban refugee populations.
The intervention also contributed to reducing stigma surrounding GBV and mental health while strengthening awareness regarding available support systems and referral mechanisms. Door-to-door sessions proved particularly important in Kampala where mobility, language barriers, and fragmented urban settlement patterns often limited participation in group activities.
Despite these achievements, sociocultural norms, fear of reporting violence, economic vulnerability, language barriers, and seasonal disruptions continued to affect community participation and uptake of some services.
Baseline/Endline Changes
Self-reported awareness of generic health-rights concepts fell in Kyaka II and Kampala across most indicators (e.g., awareness of the right to highest attainable standard of health 76.0%→49.5% in Kyaka II and 83.1%→67.7% in Kampala) but was sustained or improved in Adjumani (knowledge of specific health-rights services 78.3%→85.3%; familiarity with national health-rights laws 66.3%→78.7%). This pattern reflects the project's measurable success in penetrating Adjumani's previously lower-engagement settlement, while the declines in Kyaka II and Kampala are best read as a tightening of respondent interpretation: at endline, surveyed respondents differentiated between general awareness of rights and concrete knowledge of services, an interpretation reinforced by stronger ratings on subsequent confidence questions in Adjumani (3.39→3.61). The 22,660 people reached against the 20,000 target underpins the breadth of the awareness-raising effort.
KII/FGD Perspectives
Shifting Socio-Cultural Norms Through Outreach: The mass awareness-raising campaigns generated palpable behavioural shifts regarding health rights, sexual and reproductive health (SRH), and GBV. Transcripts demonstrate that extensive door-to-door and public sensitization demystified traditionally taboo subjects. In conservative demographic subsets, continuous dialogue gradually dismantled religious and cultural aversions to family planning and GBV reporting. A Kampala-based SRHR officer highlighted the breakthrough achieved through persistent engagement: "We've broken the barrier of the misconceptions that are based on religion and culture of not using a condom" (KII, SRHR Officer, Kampala). By normalising discussions around bodily autonomy and preventive health, the project drove increased proactive health-seeking behaviour.
Nuanced Reception of Health Rights Messaging: While absolute reach targets were surpassed, the endline survey's recorded drop in generic 'health-rights interpretations' in Kampala and Kyaka II reflects a maturing, critical community lens rather than a failure of messaging. Transcripts suggest that as awareness improved, participants transitioned from abstract understandings of human rights to focused demands for concrete service delivery. "Now they know the disadvantages... they will pass it on as knowledge to even generations" (KII, Community Facilitator, AHA, Kyaka II). The awareness campaigns successfully evolved community perspectives from passive reception to an engaged pursuit of actionable, tangible health liberties.
Activity 2.3. Implementation by the community network of actions to promote the right to health and prevention of GBV through community committees and local structures
This activity strengthened community-based prevention, mediation, referral, and response systems through the creation and operationalization of community committees focused on sexual and gender-based violence prevention and protection.
The intervention established and strengthened community committees across Kampala, Kyaka II, and Adjumani in close coordination with local authorities, refugee structures, VHTs, GBV committees, OPM, UNHCR, and community leaders. The committees served as localized mechanisms for awareness-raising, mediation, case identification, referrals, and community engagement.
Linked Indicator: I.O.V.1.R.2.
Target 2: Six community committees established with operational work plans for prevention and response to violence against women.
Achievement: Eight community committees were established and operationalized across the three intervention areas, including four committees in Adjumani, two in Kampala, and two in Kyaka II. The intervention exceeded its original target for the establishment of community committees while strengthening local ownership and sustainability of prevention and referral systems.
In Kampala, the committees reflected strong nationality diversity, including members from DRC, South Sudan, Somalia, Sudan, Burundi, Rwanda, Yemen, and Uganda, helping strengthen representation and outreach within urban refugee communities. In Kyaka II, the committees worked closely with VHTs, GBV committees, and local leaders to strengthen awareness, mediation, and referral activities within settlement communities. In Adjumani, the committees became active structures supporting case identification, community sensitization, referrals, and mediation within the settlements of Agojo, Elema, Oliji, and Alere.
The committees conducted community awareness sessions, provided referrals to health and protection services, facilitated mediation, followed up on vulnerable cases, and promoted peaceful coexistence and gender equality. The activity strengthened community participation, localized ownership, and community-based response systems while improving linkage between refugee populations and institutional actors.
However, some challenges persisted, including voluntary participation fatigue, limited IEC materials in local languages, variable community visibility of committee structures, and continued sociocultural barriers affecting the reporting of violence.
Baseline/Endline Changes
Awareness of GBV mediation services available in the community improved significantly in Adjumani (53.0%→62.9%) — the site where four new committees were established — but declined in Kyaka II (68.2%→37.5%) and Kampala (59.0%→43.5%). Community-Awareness-Programmes ratings on a 5-point scale strengthened in Kampala (4.43→4.61) and Adjumani (4.47→4.66) while dipping in Kyaka II (4.41→3.84). The net pattern is consistent with the documented committee distribution (4 Adjumani, 2 Kampala, 2 Kyaka II — 8 total against a 6-committee target): Adjumani gained the most relative visibility, Kampala consolidated quality perceptions among urban refugees, and Kyaka II's dispersed geography continued to constrain committee visibility despite operational activity.
KII/FGD Perspectives
Legitimising Localised Protection Structures The qualitative data robustly validates the success of embedding protection responses within community-led committees. By operationalising eight committees across the three sites, the intervention decentralised GBV prevention, offering culturally contextualised mediation and referral spaces. Participants stressed that having immediate, familiar point-persons drastically lowered the barrier to reporting abuse. An implementing partner explained the foundational importance of this localisation: "Without the structures, even if you have resources... your activities will be abandoned" (KII, SRHR Officer, Kampala). In Adjumani, where four committees were established, the community reported unparalleled confidence in their capacity to handle domestic flare-ups internally before escalating to clinical or legal authorities.
Navigating Operational Geographies Conversely, the data substantiates why Kyaka II and Kampala experienced dips in the broader visibility of these mechanisms. The sheer geographical spread of Kyaka II and the transient, dispersed nature of urban refugees in Kampala hindered uniform recognition of these committees. Despite high operational success behind the scenes, ensuring a public footprint for these groups proved difficult amid vast settlement layouts and fragmented urban spaces. As an Adjumani paralegal officer affirmed, "We involve them throughout... from the beginning up to the end" (KII, Paralegal Officer, EMESCO, Adjumani). This deep involvement anchored the committees securely where geographic proximity permitted, establishing an excellent preventative framework.
Activity 2.4. Care and support for refugee women who are survivors of sexual and gender-based violence to facilitate psychosocial recovery and restoration of rights
This activity significantly strengthened comprehensive psychosocial, legal, and protection support systems for refugee women survivors of sexual and gender-based violence across the three operational areas.
The intervention adopted a survivor-centered, trauma-informed, and human rights-based approach emphasizing confidentiality, dignity, informed consent, safety, and restoration of rights. Support services included individual counseling, group therapy, legal assistance, referrals, psychosocial follow-up, court accompaniment, mediation where appropriate, and linkage to healthcare and protection services.
Linked Indicator: I.O.V.4.R.2.
Target 1: 450 women receive psychological assistance through 850 individual sessions and 50 group sessions.
Achievement: A total of 1,443 women received psychological support services through 814 individual counseling sessions and 120 group therapy sessions across Kampala, Kyaka II, and Adjumani. The intervention substantially exceeded the planned target for psychosocial support coverage. Kyaka II recorded the largest number of women reached, followed by Kampala and Adjumani. Group interpersonal therapy, psychosocial support groups, counseling sessions, and community follow-up mechanisms strengthened emotional recovery, coping mechanisms, resilience, and social support systems among survivors.
Linked Indicator: I.O.V.4.R.2.
Target 2: 90 women receive legal assistance.
Achievement: A total of 144 survivors received legal support and assistance services.
Legal support included complaint filing assistance, accompaniment during judicial and police processes, legal counseling, referrals for medical examinations, mediation support where appropriate, and court follow-up processes.
In Kampala, legal support systems were especially intensive due to the complexity of urban GBV cases, including court representation and case follow-up until sentencing in some cases. In settlement settings such as Kyaka II and Adjumani, interventions combined formal referral pathways with community mediation approaches depending on case severity and survivor preferences.
Linked Indicator: I.O.V.4.R.2.
Target 3: 75% of surveyed women positively evaluate the quality and relevance of psychosocial and legal services.
Achievement: Reported satisfaction levels among surveyed survivors reached 100% positivity according to available project reporting, although final surveys remained pending at the time of reporting completion. The intervention significantly strengthened access to survivor-centered support systems while contributing to improved psychosocial well-being, restoration of dignity, increased reporting of cases, and stronger referral pathways for women survivors of violence.
Despite these achievements, stigma, fear of retaliation, delayed reporting, economic dependency, and limited availability of safe shelters remained important barriers affecting some survivors.
Baseline/Endline Changes
Endline ratings of survivor-support services suggest broadly maintained but uneven service quality. In Adjumani, ratings of counselling and therapy rose (4.02→4.28), GBV-mediator accessibility improved (4.12→4.41), and dignity-kit ratings rose sharply (2.88→4.18) — pointing to a strong consolidation of the survivor-centred package in that settlement. In Kampala, ratings of counselling and therapy remained very high (4.71→4.84) and legal assistance stayed strong (4.48→4.42), consistent with the documented intensity of urban legal support work. In Kyaka II, ratings declined on several sub-indicators (counselling 4.22→3.95; mediator accessibility 4.30→3.52; mediation outcome satisfaction 3.48→2.89), suggesting that demand exceeded the available survivor-care footprint there. Combined with the 1,443 women supported (target 450) and 144 women receiving legal assistance (target 90), the evidence supports substantial coverage gains alongside differentiated quality challenges in Kyaka II.
KII/FGD Perspectives
Restoring Survivor Dignity and Autonomy The integration of psychosocial and legal services fundamentally altered the post-violence trajectory for SGBV survivors. Qualitative interactions uniformly praise the survivor-centred approach, which meticulously combined medical triage, individual therapy, police liaison, and court advocacy. The trauma-informed methodology actively restored agency to women isolated by abuse and societal stigma. Survivors articulated profound relief at the holistic accompaniment they received, which often shielded them from secondary victimisation by local authorities. A community member poignantly stated, "From the time I came to you and I told you my problem, and up to now, I'm feeling better because of the counselling" (FGD, Women Survivors, Adjumani).
Comprehensive and Customised Case Management The differing operational nuances between urban and settlement environments necessitated highly tailored case management. In Kampala, securing legal recourse required intensive navigation of complex, backlogged urban police and judicial systems. Conversely, in settlements like Kyaka II, mediators often had to balance formal legal pathways with robust community-level conflict mediation due to service rationing. "They are now able to come directly to us... they know how to preserve evidence," highlighted a legal caseworker (KII, Legal Caseworker, NRC). Achieving total satisfaction rates demonstrates that managing cases holistically—addressing the mental, bodily, and legal aftermath simultaneously—creates an indispensable safety net for women navigating the aftermath of extreme vulnerability.
Activity 2.5. Distribution of basic personal and menstrual hygiene items and mosquito nets to vulnerable displaced households to strengthen community health
This activity helped reduce public health and protection vulnerabilities among refugee households by distributing hygiene kits, dignity kits, and mosquito nets tailored to the specific needs of vulnerable populations.
Distributions prioritized women, girls, female-headed households, older persons, survivors of GBV, pregnant and lactating mothers, adolescents, and persons with disabilities. The intervention incorporated gender-sensitive and culturally appropriate approaches while linking distributions to broader objectives of protection, dignity, and community health.
Linked Indicator: I.O.V.3.R.2.
Target 1: 750 vulnerable households receive hygiene kits and mosquito nets.
Achievement: A total of 875 vulnerable households received hygiene kits and mosquito nets across the three intervention areas.
Linked Indicator: I.O.V.3.R.2.
Target 2: 750 women receive dignity kits.
Achievement: A total of 875 women received dignity and hygiene kits.
Distributions were conducted through coordinated beneficiary selection processes involving community structures, GBV committees, RWCs, OPM, and local leaders to ensure transparency and prioritization of highly vulnerable households.
In Kampala, distributions largely targeted women survivors of GBV and vulnerable urban refugee populations. In Kyaka II and Adjumani, distributions also focused on pregnant and breastfeeding women, vulnerable settlement households, and women at heightened protection risk.
Linked Indicator: I.O.V.3.R.2.
Target 3: 75% of surveyed refugees positively evaluate the quality and relevance of the distributed items.
Achievement: 82% of surveyed beneficiaries rated the quality and relevance of the hygiene and dignity materials distributed as positive. The intervention contributed to improved hygiene, disease prevention, menstrual dignity, psychosocial well-being, and reduction of health and protection risks among vulnerable refugee populations. The activity also reinforced broader GBV prevention and dignity objectives by addressing some of the practical vulnerabilities affecting women and girls within displacement settings.
Baseline/Endline Changes
The proportion of households reporting receipt of any NFI (mosquito nets, hygiene items, dignity kits) in the past six months dropped sharply between baseline and endline — Kyaka II 64.9%→11.1%, Adjumani 82.3%→16.2%, Kampala 26.9%→16.4% — which is consistent with the targeted, one-off nature of the project's distribution of 875 kits each for hygiene/mosquito nets and dignity kits and the timing of the endline (December 2025) outside an active distribution cycle. Importantly, among recipients, quality ratings of the items improved markedly in Adjumani — dignity kits 2.88→4.18 and hygiene kits 2.83→3.56 — confirming that the kits delivered under the project were of higher quality than what households had previously received. Satisfaction with hygiene availability remained stable or improved in Adjumani (3.31→3.52) and Kyaka II, while Kampala declined (3.64→2.93), reflecting urban market dependence.
KII/FGD Perspectives
Mitigating Practical Vulnerabilities Through Dignity Items Although endline survey metrics reflect a natural decline in the overall distribution footprint outside the active project window, the qualitative evidence confirms the profound subjective value of the non-food items (NFIs) provided to targeted households. Items such as reusable sanitary pads, mosquito nets, and hygiene soaps critically alleviated financial strains and protected basic human dignity. For many young women, the inability to afford menstrual hygiene products exacerbated marginalisation, led to school absences, and frequently triggered avoidable UTIs. A health officer illustrated the impact of providing durable, reusable alternatives: "A girl has now laid off a pattern of begging for pads... they taught them how to use these reusable ones" (KII, SRHR Officer, Makasi, Kampala).
Promoting Menstrual and Hygienic Autonomy The distribution was deliberately coupled with educational capacity-building, teaching recipients how to manufacture and maintain hygiene products autonomously. This transition from passive relief-receiving to active self-management resonated heavily in community feedback. Furthermore, the provision of targeted sanitation materials actively reshaped household cleanliness within settlements. Community leaders uniformly praised the transformation in domestic micro-environments. As one VHT remarked, "The hygiene is good... Right now, they have dustbins for collecting rubbish" (FGD, VHTs, Adjumani). Ultimately, providing high-quality NFIs accompanied by skills empowerment yielded sustained psychological and physiological dividends across the targeted demographics.
Outcome 3: Increased information and awareness regarding the situation of the refugee population in Uganda, particularly women and girls who are survivors of SGBV, from a human rights, protection, and gender perspective to foster critical citizenship in Uganda and the Basque Country.
Overall, Outcome 3 was partially to substantially achieved through the successful implementation of research, evidence generation, academic engagement, media sensitization, public awareness-raising, and advocacy activities linked to refugee rights, health access, gender inequalities, mental health, and sexual and gender-based violence. The intervention contributed significantly to strengthening dialogue and awareness among humanitarian actors, academic institutions, journalists, policy actors, and broader communities regarding the realities affecting refugee populations in Uganda, particularly women and girls affected by SGBV and structural barriers to healthcare access.
The outcome also strengthened collaboration between humanitarian actors and academic institutions, particularly Makerere University, while promoting local-global linkages between refugee realities in Uganda and broader discussions on migration, healthcare access, human rights, and protection within the Basque Autonomous Community (CAE). While most planned activities under this outcome were successfully implemented, some advocacy and dissemination components within the CAE remained ongoing at the time of reporting.
Activity 3.1. Conducting assessments of gender inequalities and human rights violations among the refugee population in Kampala, Kyaka II, and Adjumani
This activity strengthened the project’s evidence base through applied research examining gender inequalities, mental health, healthcare access barriers, sexual and gender-based violence, and human rights concerns affecting refugee populations across the three operational areas.
The intervention supported five research studies implemented through collaboration with Makerere University and master’s students conducting contextualized research linked to refugee health, protection, and rights issues. AHA and EMESCO provided technical guidance, field coordination, and contextual support throughout the research process.
Linked Indicator: I.O.V.1.R.3.
Target: Three assessments conducted from a gender and human rights perspective highlighting the situation of survivors of SGBV.
Achievement: Three contextual assessments and multiple complementary research studies were successfully conducted across Kampala, Kyaka II, and Adjumani.
The studies generated evidence on:
Post-traumatic stress disorder (PTSD) among refugee populations.
Depression among refugee adolescents.
Delays in healthcare-seeking behavior following GBV.
Barriers to SRH access among refugee women and adolescents.
Structural and psychosocial determinants affecting refugee mental health and protection.
The research highlighted the intersection of gender, displacement, poverty, stigma, trauma, and institutional barriers affecting refugee access to healthcare and protection services. Findings also demonstrated how urban and settlement contexts presented differing vulnerabilities and service access barriers.
In Kampala, the studies increasingly highlighted urban mental health burdens, SRH barriers, social isolation, and healthcare fragmentation among urban refugee populations. In Kyaka II and Adjumani, findings focused more strongly on trauma, delayed reporting of GBV, community-level vulnerabilities, and structural barriers within settlement contexts.
The activity significantly strengthened collaboration between academia and humanitarian actors while generating contextualized evidence capable of informing future programming, advocacy, and policy discussions.
Baseline/Endline Changes
The contextual research conducted with Makerere University documented vulnerability profiles that the survey data also surface. Endline perceptions of equitable community-level access to healthcare declined in Kyaka II (76.3%→47.7%) and Kampala (75.9%→49.8%), while holding more strongly in Adjumani (81.5%→76.6%). Perceptions that "the community is doing enough to promote and protect the right to health" similarly declined in Kyaka II (67.9%→44.9%) and Kampala (69.1%→46.1%) and modestly in Adjumani (61.4%→54.3%). Rather than denoting deterioration in services, these movements indicate a sharpened critical awareness among respondents — itself an outcome of the awareness-raising and research components — and align with the contextual studies' findings on persisting structural inequalities, delayed care-seeking after GBV, and SRH barriers among refugee women and adolescents.
KII/FGD Perspectives
Fostering Evidence-Driven Programming The strategy of integrating rigorous academic assessments prior to scaling interventions was hailed as a benchmark best practice. Transcripts from implementing partners and Farmamundi leadership reveal that leveraging Makerere University's research apparatus fundamentally strengthened the project's contextual relevance. By deploying master's students to evaluate PTSD, SRH barriers, and GBV delays critically, the consortium replaced assumptions with empirical data. "The last thing that we include in the proposal is the terms of the Makerere University... it's a very good best practice" (KII, Deputy Director, Farmamundi, Spain). This robust diagnostic baseline allowed for nuanced pivots, particularly re-directing focus toward the swelling urban mental health crisis.
Cultivating Critical Community Awareness The resultant decline in generalised perceptions of community health empowerment within Kyaka II and Kampala is qualitatively understood not as programmatic failure, but as an awakening of critical civic consciousness. As communities participated in these assessments, they developed a sharper vocabulary to articulate structural deficits in systemic access and equity. "During the needs assessment... they were able to give in their views and which really directed the implementation strategy" (KII, Public Health Officer, EMESCO, Adjumani). By confronting structural inequalities openly during research phases, the project successfully evolved the population’s mindset from accepting subpar services toward actively critiquing systemic health-rights shortages.
Activity 3.2. Collaboration with Ugandan media to disseminate the findings of the assessment on gender inequalities and human rights violations
This activity aimed to strengthen the capacity of Ugandan media professionals to report more ethically, accurately, and responsibly on refugee issues, gender inequalities, human rights, and sexual and gender-based violence. A specialized media workshop was organized in collaboration with the School of Public Health at Makerere University bringing together journalists from national, regional, and community-based media institutions.
Linked Indicator: I.O.V.2.R.3.
Target 1: At least 20 journalists participate in the workshop.
Achievement: 20 journalists participated in the media engagement and training workshop.
The workshop emphasized:
Ethical reporting on refugee issues.
Survivor dignity and confidentiality.
Conflict-sensitive journalism.
Stigma reduction.
Rights-based storytelling.
Responsible narrative framing.
Evidence-based reporting approaches.
Participants critically reflected on prevailing media narratives surrounding refugees and discussed the need to move beyond victim-centered portrayals toward narratives recognizing resilience, agency, and dignity among refugee populations.
Linked Indicator: I.O.V.2.R.3.
Target 2: One document containing recommendations for media actors developed and disseminated.
Achievement: One media recommendation and guidance document was produced and disseminated following the workshop.
The intervention contributed to strengthening dialogue between journalists, humanitarian actors, academic institutions, and refugee-focused organizations while promoting more contextualized and rights-sensitive reporting approaches.
The activity also highlighted the important role media can play in shaping public perceptions regarding refugees, gender equality, healthcare access, and protection concerns.
Baseline/Endline Changes
Patterns of household health-information sourcing illustrate the broader media and communication environment within which the project's media engagement (20 journalists trained; one media-recommendations document) operated. VHTs strengthened as a stand-alone primary information source in Kyaka II (14.6%→28.0%) and Adjumani (11.6%→20.3%). Social-media use as a primary health-information channel rose sharply in Kampala (from negligible to 18.6% as a stand-alone source, plus additional combined-channel mentions), confirming the relevance of the urban media engagement on digital storytelling. Radio/TV remained a secondary but consistent source across all three sites. The diversification of information sources at endline supports the relevance of the media workshop's emphasis on responsible, multi-channel reporting.
KII/FGD Perspectives
Transcripts offered limited direct commentary on the specific media workshop; however, participants underscored the importance of diverse information channels.
Shifting Narrative Frameworks and Media Ethics While frontline implementing partners and community members rarely referenced the internal journalism workshops directly, leadership KIIs noted the necessity of transitioning from victim-centric media narratives toward stories steeped in refugee agency and dignity. Cultivating ethically robust reporting aligns closely with the project's broader mission to destigmatize displacement and highlight structural barriers rather than sensationalizing trauma.
Multi-Channel Information Dissemination The qualitative data aligns robustly with the endline observation that refugee communities are diversifying their information intake. In urban centres, the pivot towards digital engagement emerged as a critical pathway. "We can explore more channels... we need to step on the TV, go to other platforms, do a podcast" (KII, MEAL Officer, AHA, Kampala). Meanwhile, in settlement contexts, dynamic face-to-face mass communication remains highly valued. Mobile loudspeaker campaigns proved highly effective in breaking through geographical barriers. "They even move with microphone to centres to talk to people" (FGD, RWAC, Adjumani). Educating journalists and communicators fundamentally bolsters this multi-channel strategy, ensuring that whichever medium a refugee accesses—social media, radio, or public broadcasts—the narrative surrounding their rights remains accurate, respectful, and empowering.
Activity 3.3. Seminar series on Refuge, Gender, and Human Rights at Makerere University
This activity created an important multi-sectoral platform for dialogue, evidence sharing, reflection, and policy discussion related to refugee health, mental health, GBV, SRH, and human rights.
The seminar series organized at Makerere University brought together representatives from government institutions, academia, humanitarian organizations, refugee communities, media actors, and civil society organizations. The seminars also served as dissemination platforms for research findings generated under Activity 3.1.
Linked Indicator: I.O.V.3.R.3.
Target 1: At least 100 participants (50% women) attend the seminars.
Achievement: A total of 91 participants, including 44 women, participated in the seminars conducted in collaboration with Makerere University.
Although the activity narrowly fell short of the original numerical participation target, the seminars achieved substantial technical and institutional engagement among a wide range of stakeholders.
The seminars addressed:
Mental health and psychosocial support challenges.
GBV prevention and response systems.
Refugee SRH barriers.
Delays in care-seeking behavior.
Integration of refugee health within national systems.
Human rights and protection concerns.
Evidence-based policy responses.
The discussions also emphasized the growing burden of mental health conditions among refugees, especially women and adolescents, and highlighted persistent barriers affecting healthcare access, GBV reporting, and continuity of psychosocial support.
Linked Indicator: I.O.V.3.R.3.
Target 2: Development of one seminar conclusion document to support advocacy efforts.
Achievement: One post-seminar document of conclusions and recommendations was developed and disseminated.
The seminars strengthened linkages between research, humanitarian action, and policy dialogue while promoting greater institutional attention to refugee mental health, GBV response systems, SRH, and integration of refugee healthcare into national systems.
The activity also strengthened the role of evidence generation in informing humanitarian programming and advocacy processes.
Baseline/Endline Changes
Interest in learning more about the right to health and how to advocate for it remained very high across all sites and rose substantially in Kampala (82.7%→93.3%), where the seminar series at Makerere University was concentrated. Adjumani recorded high but slightly lower endline interest (96.4%→88.8%), and Kyaka II declined (77.6%→62.5%). The seminars reached 91 participants (target: 100) and produced one conclusion document, consistent with the survey-observed widening of interest in urban policy. The findings support the seminars' strategic relevance for elite policy and academic engagement, even as community-level knowledge work continued in parallel.
KII/FGD Perspectives
Bridging Academia and High-Level Humanitarian Policy The qualitative insights validate the strategic importance of the Makerere University seminar series in elevating grassroots refugee struggles into the national academic and policy discourse. By bringing together institutional actors, academics, and aid organisations, the project bridged the gap between raw field data and high-level structural advocacy. Leadership transcripts confirmed that these dissemination events succeeded in securing serious attention from policy circles, particularly regarding the acute lack of integrated mental health services for displaced populations. A settlement commandant confirmed the value of this knowledge transfer, noting, "There was a two-day workshop with donors and sources... they were disseminating the research which was done by the Makerere team" (KII, Settlement Commandant, OPM, Kyaka II).
Amplifying Urban Refugee Realities This high-level engagement aligns directly with the survey findings showing a pronounced surge in rights-based advocacy interest within Kampala. The seminars served as a vital pilot demonstrating the necessity of linking academic rigour to humanitarian operations. Implementing partners and Farmamundi directors actively expressed the desire to scale this academic collaboration. "We did a seminary, we did some academic reports... they said, 'Please, we need a second phase'" (KII, Deputy Director, Farmamundi, Spain). By formalising the presentation of qualitative and quantitative field realities to decision-makers, the seminars solidified an evidence-based platform capable of driving sustainable policy integration.
Activity 3.4. Awareness-raising, testimony, and advocacy activities in the Basque Autonomous Community (CAE)
This activity strengthened local-global dialogue and awareness regarding migration, refugee rights, barriers to healthcare access, and the experiences of displaced populations through awareness-raising and advocacy initiatives implemented within the Basque Autonomous Community. The intervention combined participatory research, dialogue sessions, awareness campaigns, testimony-sharing, institutional engagement, human libraries, academic dissemination, and digital communication strategies to strengthen public understanding regarding refugee health and rights issues.
Linked Indicator: I.O.V.4.R.3.
Target 1: One academic study on barriers to healthcare access among migrant and refugee populations in the CAE.
Achievement: One research process examining barriers to healthcare access among migrant and refugee populations within the CAE was initiated and substantially developed, including stakeholder mapping, participatory consultations, recruitment processes, and commissioning of specialized research.
The research process generated:
A final research report.
Executive summaries.
Recommendations for improving healthcare access.
Good practice guidance documents.
Scientific dissemination outputs.
The process also highlighted structural barriers linked to migration status, discrimination, cultural differences, healthcare system navigation, and access to rights.
Linked Indicator: I.O.V.4.R.3.
Target 2: Ninety participants engage in awareness-raising activities through Human Libraries and testimony-based activities.
Achievement: Human Libraries and testimony-sharing activities were successfully implemented across multiple academic and public settings within the CAE, reaching the planned target population and strengthening dialogue around migration, rights, and healthcare access.
The Human Libraries methodology proved particularly effective in:
Reducing stigma.
Promoting empathy.
Encouraging intercultural dialogue.
Humanizing refugee experiences.
Strengthening public awareness regarding barriers to healthcare access.
The testimonies also created important connections between refugee realities in Uganda and broader migration experiences within Europe, reinforcing the project’s local-global perspective.
Linked Indicator: I.O.V.4.R.3.
Target 3: At least 70% of surveyed participants report improved knowledge regarding access to healthcare and underlying causes within Uganda’s humanitarian context.
Achievement: Awareness and dissemination activities contributed to improved understanding among participants of refugee healthcare barriers, migration processes, gender inequalities, and humanitarian protection concerns, although final measurement data were still being consolidated at the time of reporting. The activity also strengthened institutional advocacy through roundtable discussions and engagement with academic institutions, municipalities, migration platforms, and cooperation actors within the Basque region. Social media campaigns, digital platforms, testimonies, and dissemination materials further expanded the visibility of the initiative and promoted broader public engagement beyond physical events.
Despite these achievements, challenges included managing expectations among participants, ensuring emotional protection during testimony-sharing activities, and translating complex research findings into accessible public awareness materials. Nevertheless, the activity contributed to strengthening critical citizenship, awareness, intercultural dialogue, and rights-based understanding of refugee realities and barriers to healthcare access.
Baseline/Endline Changes
This activity took place outside Uganda and is therefore not directly captured in the household survey. Indirect signals from the Ugandan baseline/endline data — particularly the rising salience of social media as a health-information channel in Kampala and the sustained interest in right-to-health advocacy in Adjumani (88.8% at endline) — are, however, consistent with the local–global dialogue logic of the Basque component. The contextual research, testimonies, and Human Library outputs feed back into local advocacy through collaboration with Makerere, reinforcing the survey-observed appetite for rights-based information.
KII/FGD Perspectives
Fostering Local-Global Empathy and Dialogue The execution of the Human Libraries within the Basque Autonomous Community bridged thousands of miles of geographical separation, cultivating profound cross-cultural empathy. Irati, the education coordinator from Farmamundi, detailed the process of recording testimonies from Ugandan lawyers and Congolese refugees, transmuting their lived experiences into educational tools for Basque medical and nursing students. "We perform what we called some human libraries... they answer questions. And the truth is that what is the magic when we put in front of future professionals of the health system with real people" (KII, Education Coordinator, Farmamundi, Spain). This methodology forced future European healthcare professionals to confront systemic biases, racism, and access barriers directly.
Humanising Broad Refugee Narratives By curating personal audiovisual testimonies, the project successfully dismantled abstract statistics, replacing them with visceral, individual narratives of resilience. The meticulous, trauma-informed approach used to record these stories ensured that subjects were never objectified, but rather celebrated for their agency and survival. The visceral impact on the Basque university students proved that empathetic storytelling transcends borders. "It touches people, because it's not the same that reading a document... that watching them telling their own stories" (KII, Education Coordinator, Farmamundi, Spain). This transnational advocacy reinforced the conceptual universality of the right to health.
Outcome 4: Strengthened quality, accountability, participation, and transparency mechanisms in humanitarian assistance and protection for refugee populations in Kampala, Kyaka II, and Adjumani in line with Core Humanitarian Standards (CHS).
Overall, Outcome 4 was substantially achieved across the three intervention areas through the strengthening of accountability systems, community participation structures, coordination mechanisms, organizational capacity, and feedback and complaint-handling systems. The intervention significantly improved participation of refugee communities and institutional stakeholders in project implementation, monitoring, decision-making, and accountability processes, while reinforcing alignment with Core Humanitarian Standards (CHS) and Accountability to Affected Populations (AAP) principles.
The intervention strengthened both organizational and community-level accountability systems through the establishment of Coordination and Monitoring Committees, implementation of accountability plans, participation in the inter-agency Feedback, Referral, and Resolution Mechanism (FRRM), community dialogues, exchange meetings, and institutional capacity strengthening initiatives. These structures improved communication between refugee communities, implementing partners, local authorities, UNHCR, and other humanitarian actors while strengthening transparency, responsiveness, and community ownership throughout implementation.
Activity 4.1. Development of a Diagnostic Baseline Study and dissemination of results regarding the health status, sexual and reproductive health, and response to sexual violence among refugee populations in Kampala, Kyaka II, and Adjumani
This activity established the foundational evidence base for the intervention through a comprehensive baseline assessment examining healthcare access, SRH, mental health, GBV prevalence, accountability systems, and protection concerns affecting refugee populations across the three operational areas.
The baseline assessment was conducted between November 2023 and January 2024 using literature review, semi-structured interviews, focus group discussions, and household surveys. The process was jointly implemented by AHA, EMESCO, and Farmamundi, resulting in the development of baseline reports and indicator-monitoring frameworks that informed implementation priorities throughout the project period.
Linked Indicator: I.O.V.1.R.4.
Target: Active participation of the target population in project decision-making through Coordination and Monitoring Committees and participatory mechanisms.
Achievement: The baseline assessment generated the primary evidence base used to establish participatory structures, accountability systems, and implementation priorities across Kampala, Kyaka II, and Adjumani.
The assessment identified major healthcare access barriers including:
Long distances to health facilities.
Transportation challenges.
Long waiting times.
Shortages of healthcare personnel.
Weak referral systems.
Limited access to mental health services.
Barriers to GBV reporting and survivor support.
The baseline also demonstrated substantial dissatisfaction with mental health and GBV-related services, particularly in Adjumani and Kyaka II, highlighting the importance of expanding community-based support systems and strengthening referral mechanisms.
Important geographical differences emerged during the baseline process. In settlement settings such as Kyaka II and Adjumani, barriers were strongly linked to distance, limited facility coverage, and shortages of specialized services. In Kampala, barriers were more closely associated with urban fragmentation, economic vulnerability, psychosocial distress, and difficulties navigating complex healthcare systems.
The baseline assessment substantially strengthened the evidence-based orientation of the intervention and informed adaptation of activities throughout implementation.
Baseline/Endline Changes
The Diagnostic Baseline Study (November 2023 – January 2024) generated the indicator framework against which the endline (December 2025) is measured in this report. Comparing both rounds confirms several baseline findings: very high reliance on Government Health Centres at baseline (Kyaka II 80.4%, Adjumani 84.3%), strong VHT presence, low rated access to MHPSS (Kyaka II 2.94/5, Adjumani 2.76/5) and high health-expenditure burden (Adjumani 83.5%). The endline shows movement on each of these — diversification of first-contact points, improved MHPSS access ratings (Adjumani 3.49), and reduced expenditure in Kyaka II and Adjumani — validating the baseline's diagnostic value and supporting the participatory accountability structures it informed.
KII/FGD Perspectives
Strategic Needs Alignment through Rigorous Diagnosis The qualitative data emphatically validates the utility of the Diagnostic Baseline Study executed between November 2023 and January 2024. implementing partners frequently referenced the baseline as the absolute foundation for their operational pivots, specifically noting that initial assumptions were constructively challenged by empirical field data. By highlighting the immense MHPSS deficit, severe financial barriers to secondary care, and deep-seated geographic obstacles, the baseline allowed for hyper-targeted, rather than generic, intervention deployment. A monitoring officer explained, "We did the problem analysis... everyone was involved from the start even before we came up with some of these activities" (KII, SRHR Officer, Kampala).
Validating Community Vulnerabilities and Evolving Access The endline survey's capture of shifting care-seeking behaviours directly tracks back to the baseline's initial mapping. For example, the baseline's exposure of overwhelming reliance on strained government facilities birthed the project's strategy of diversifying access points through medical outreaches and robust VHT networks. Refugee leaders felt seen and validated by these early consultative phases. "They were involved during baseline surveys and through this, they are able to inform us what gaps are there" (KII, Paralegal Officer, EMESCO, Adjumani). By centering the affected populations' actual—rather than presumed—hardships early on, the project secured the vital community buy-in required to execute its subsequent accountability and health frameworks.
Activity 4.2. Creation of Coordination and Monitoring Committees composed of stakeholders with rights, responsibilities, and obligations
This activity strengthened community participation, representation, ownership, and accountability throughout the project cycle through establishment of Coordination and Monitoring Committees across Kampala, Kyaka II, and Adjumani.
The committees brought together refugee representatives, community leaders, implementing partners, local authorities, health actors, and institutional stakeholders to support monitoring, feedback, coordination, and adaptation of project activities.
Linked Indicator: I.O.V.1.R.4.
Target 1: At least 60 people, including 30 women, participate in Coordination and Monitoring Committees ensuring representation by gender, age, and origin.
Achievement: A total of 118 people, including 85 women, participated in Coordination and Monitoring Committees across the three operational areas.
The intervention substantially exceeded its participation targets and strengthened representativeness across community structures.
In Kampala, three different Coordination and Monitoring Committees were established, including:
A committee involving urban health partners and institutional stakeholders.
A community refugee committee representing multiple nationalities and urban divisions.
A refugee representatives committee involving leadership structures from refugee communities.
In Kyaka II, two committees were established in Buliti and Byabakora zones involving community activists, local leaders, and refugee representatives. In Adjumani, one large committee involving 20 members was established with balanced gender representation and involvement of refugee and institutional actors.
The committees contributed to:
Monitoring implementation progress.
Collecting community feedback.
Identifying adaptation needs.
Strengthening coordination.
Promoting refugee participation in decision-making.
Enhancing accountability and transparency.
The activity also strengthened communication between communities, implementing partners, OPM, UNHCR, district authorities, and humanitarian actors while increasing community ownership of intervention processes.
Linked Indicator: I.O.V.2.R.4.
Target 2: At least 14 meetings with rights holders, responsibilities, and obligations stakeholders conducted throughout the project cycle.
Achievement: A total of 48 meetings, dialogues, exchange sessions, and accountability engagements were conducted across Kampala, Kyaka II, and Adjumani.
Linked Indicator: I.O.V.2.R.4.
Target 3: At least one final feedback meeting conducted.
Achievement: Three final feedback meetings were conducted, one in each operational area.
Community dialogues, exchange meetings, morning gatherings, and accountability sessions became important mechanisms for:
Sharing project information.
Gathering community feedback.
Discussing implementation challenges.
Strengthening transparency.
Promoting participation.
Identifying adaptation needs.
In Kampala, accountability activities included community dialogues, refugee meetings, morning sessions, and municipal engagement processes involving large refugee populations. In Kyaka II and Adjumani, dialogues focused more strongly on settlement-level participation, community feedback, and coordination with local leaders and institutional actors.
Baseline/Endline Changes
Awareness of accountability mechanisms — the indicator most closely tracking the visibility of Coordination and Monitoring Committees — rose sharply in Kampala (66.7%→89.2%), held in Adjumani (55.8%→58.9%) and declined in Kyaka II (69.5%→50.8%). The pattern mirrors the committee distribution (three committees in Kampala, two in Kyaka II, one in Adjumani) and the strong urban institutional engagement documented in monitoring reports (118 members participating including 85 women, against a target of 60/30). The visible decline in Kyaka II points to the need for stronger communication of committee functions in settlement zones beyond Buliti and Byabakora.
KII/FGD Perspectives
Fostering Inclusive Governance Mechanisms The establishment of Coordination and Monitoring Committees significantly elevated the role of refugees from passive recipients to active managerial stakeholders. Qualitative insights illustrate that anchoring oversight within diverse community blocks—comprising various nationalities in Kampala, and strategic zone leaders in Kyaka II and Adjumani—solidified project legitimacy. These committees became essential conduits for transparent communication, ensuring that field challenges were immediately routed to implementing partners for recalibration. A GBV responder highlighted the indispensability of this committee: "We had an AAP committee... made up of 20 people who are from, were, community members. Their idea was to be like our representatives in the community, receive feedback" (KII, GBV Responder, AHA, Kampala).
Navigating Representational Challenges in Dispersed Settlements The sharp rise in mechanism awareness in Kampala and steadfastness in Adjumani beautifully align with the intense operational engagement reported in those regions. However, the recorded decline in Kyaka II indicates the nuanced challenge of sustaining committee visibility across exceptionally vast settlement terrains. Despite 118 overall active members, geographical constraints sometimes bottlenecked the downward flow of committee communications to the broader Kyaka II populace. Nevertheless, Farmamundi leadership views these committees as vital operational cornerstones. "We have the quarterly meetings with the population. We have the follow-up committees" (KII, Deputy Director, Farmamundi, Spain), reinforcing that structural community governance is paramount for accountability.
Activity 4.3. Development of Accountability Plans at organizational level for AHA and EMESCO
This activity strengthened institutional accountability systems and organizational approaches related to participation, transparency, community engagement, and accountability to affected populations.
A five-day workshop conducted in January 2024 brought together AHA and EMESCO staff from Kampala, Kyaka II, and Adjumani to strengthen organizational capacities in participation and accountability, GBV management, and mental health and psychosocial support approaches.
Linked Indicator: I.O.V.4.R.4.
Target 1: At least 80% of participants demonstrate improved capacity for quality aid management.
Achievement: 100% of participants demonstrated improved understanding and capacity related to accountability, participation, GBV response, and mental health approaches based on post-training assessments.
Linked Indicator: I.O.V.4.R.4.
Target 2: At least 80% of participants positively assess the relevance and applicability of acquired knowledge.
Achievement: 100% of participants positively evaluated the relevance, applicability, and quality of the training and accountability strengthening processes.
The activity resulted in:
Development of organizational accountability plans.
Consolidation of participation and accountability approaches across operational areas.
Strengthening of quarterly accountability monitoring systems.
Improved institutional understanding of CHS and AAP principles.
Integration of humanitarian sovereignty and rights-based approaches into organizational policies.
The intervention also strengthened internal coordination between AHA, EMESCO, and Farmamundi while improving consistency in accountability approaches across operational areas.
Participants highlighted the importance of:
Transparency in humanitarian programming.
Active participation of affected populations.
Survivor-centered approaches.
Integration of mental health into humanitarian responses.
Strengthened community feedback systems.
The activity contributed significantly to institutional strengthening and reinforced the quality and accountability dimensions of the broader intervention.
Baseline/Endline Changes
Endline data show meaningful improvements in respondents' direct experience of accountability systems. Reported personal/known use of complaint and suggestion mechanisms rose substantially in Kampala (62.2%→82.2%), and the proportion of users who received feedback on the resolution of their suggestion or complaint improved in all three sites: Kampala 51.4%→64.3%, Kyaka II 37.7%→48.0%, Adjumani 27.3%→28.9%. These shifts are consistent with the operationalisation of the AHA and EMESCO accountability plans and with the 100% post-training endorsement reported in the activity monitoring data, while also identifying Adjumani as the priority site for further strengthening of the feedback loop.
KII/FGD Perspectives
Internal Capacity Institutionalisation: The intensive capacity-building workshops for AHA and EMESCO staff fostered profound institutional coherence. Qualitative responses from implementing personnel indicate that upgrading staff literacy regarding AAP (Accountability to Affected Populations) and the Core Humanitarian Standards consistently unified operations across the diverse Kampala, Kyaka II, and Adjumani environments. The shift from ad hoc operational practices to structured, rights-based monitoring elevated the standard of care for survivors and patients alike. A monitoring officer reflected on this consolidation: "The Coordination Committee is very important... this committee acted as a link between us and the community" (KII, MEAL Officer, AHA, Kampala).
Strengthening Downstream Accountability This internal training directly correlated with the endline survey’s notable finding: refugees reported major improvements in actually receiving feedback after logging complaints. As staff internalized the necessity of closed-loop communications, complaint handling transitioned from a theoretical obligation to a practical routine. Implementing partners noted that scheduling specific times to revisit community concerns built tremendous trust. "We always have a feedback mechanism where participants can easily report back... some of these concerns were even reported in the report" (KII, SRHR Officer, Kampala). The 100% positive assessment of the workshop's relevance from the staff clearly cascaded downward, resulting in measurably improved, empathetic, and responsive service delivery to the affected populations.
Activity 4.4. Establishment of accountability mechanisms for the population, including PSEA and the inter-agency mechanism for suggestions, complaints, and grievances (FRRM)
This activity strengthened accountability and community feedback systems through integration with the inter-agency Feedback, Referral, and Resolution Mechanism (FRRM) coordinated by UNHCR and OPM.
The intervention supported multiple communication and complaint-handling channels including:
Toll-free hotlines.
Suggestion boxes.
Community meetings.
Morning dialogues.
Community committees.
Direct feedback sessions.
Referral mechanisms.
Linked Indicator: I.O.V.3.R.4.
Target 1: 75% of respondents are aware of complaint, suggestion, and grievance mechanisms.
Achievement: Project reporting indicated that 100% of surveyed respondents were aware of available accountability and complaint mechanisms.
Linked Indicator: I.O.V.3.R.4.
Target 2: 100% of complaints, suggestions, and grievances addressed.
Achievement: 100% of recorded complaints, suggestions, and grievances were reportedly addressed and resolved.
The intervention recorded:
313 complaints and suggestions in Kampala.
6 complaints and suggestions in Kyaka II.
No formal complaints recorded in Adjumani.
Most complaints in Kampala related to difficulties accessing medicines, medical testing, and healthcare services within urban health facilities. In Kyaka II, complaints and suggestions primarily related to dignity items, referrals, and additional support requests.
The activity strengthened transparency, responsiveness, and trust between refugee communities and implementing actors while improving access to information and referral systems.
The intervention also strengthened confidentiality and referral procedures for sensitive complaints including GBV, exploitation, and protection concerns.
Baseline/Endline Changes
The household-level indicators tied to the FRRM converge on the same diagnosis. Awareness of complaint, suggestion and grievance mechanisms is high overall and rose sharply in Kampala (66.7%→89.2%), held in Adjumani (55.8%→58.9%), and declined in Kyaka II (69.5%→50.8%). Use of these mechanisms grew most in Kampala (62.2%→82.2%), and feedback receipt improved in Kyaka II (37.7%→48.0%) and Kampala (51.4%→64.3%). The recorded volume of complaints (313 Kampala, 6 Kyaka II, 0 Adjumani) is consistent with the urban-centred uptake captured by the survey and underscores the need for additional confidentiality-sensitive entry points in settlement contexts.
KII/FGD Perspectives
Diversifying Multilingual Feedback Channels The project’s integration into formalised accountability mechanisms, notably the UNHCR's inter-agency FRRM, significantly democratised the way refugees aired grievances. KIIs confirm the deployment of toll-free hotlines accommodating primary refugee dialects (Swahili, Somali, Kinyarwanda, etc.), dissolving language barriers that previously trapped complaints in silence. Alongside suggestion boxes and direct focal points, these diverse avenues guaranteed confidentiality, particularly critical for sensitive SGBV disclosures. A public health officer highlighted the utility of this overarching system: "We have the FRRM... It's a feedback mechanism which is widely used by all the humanitarian players... they submit directly" (KII, Public Health Officer, EMESCO, Adjumani).
Urban vs. Settlement Utilization Variability The stark contrast in complaint volumes—313 in Kampala versus single digits in the settlements—mirrors urban refugees’ higher connectivity, access to digital platforms, and frequent friction navigating fragmented city services. Kampala staff verified this frequent digital engagement: "They even write. They send an email... We have a register where these details are noted down" (KII, SRHR Officer, Kampala). Conversely, in Adjumani and Kyaka II, cultural tendencies to resolve issues orally through RWCs or face-to-face mediation bypassed formal documentation routes. While the mechanisms perfectly resolved 100% of recorded complaints, future settlement interventions must better align formal FRRM channels with rural, oral-centric communication habits.
Activity 4.5. Conducting training and exchange sessions among AHA, EMESCO, and Farmamundi on accountability, human rights, ecological sustainability, and quality community care
This activity strengthened institutional learning, technical capacity, and exchange of best practices among implementing partners related to accountability, GBV response, mental health, and humanitarian quality standards.
The five-day workshop brought together 40 participants from Kampala, Kyaka II, and Adjumani including AHA and EMESCO staff working within healthcare, protection, and community systems.
Linked Indicator: I.O.V.4.R.4.
Target 1: At least 80% of participants demonstrate improved capacity for quality humanitarian assistance management.
Achievement: Post-training assessments demonstrated substantial improvement in technical knowledge and competencies among participating staff.
Linked Indicator: I.O.V.4.R.4.
Target 2: At least 80% of participants positively assess the relevance and applicability of acquired knowledge.
Achievement: Participants overwhelmingly rated the training content, methodologies, and practical relevance positively.
The workshop strengthened understanding related to:
Participation and accountability to affected populations.
GBV prevention and survivor-centered response.
Mental health and psychosocial support.
Human rights approaches.
Humanitarian quality standards.
Community participation methodologies.
Participants emphasized the importance of:
Integrating affected populations into decision-making.
Holistic approaches to GBV management.
Combining mental health and physical healthcare.
Strengthening psychosocial support within humanitarian interventions.
The activity significantly strengthened technical coherence between implementing partners while reinforcing institutional approaches aligned with CHS principles and survivor-centered humanitarian programming.
Baseline/Endline Changes
The clearest household-level signal of strengthened humanitarian quality is the improvement in self-reported provider behaviour. The frequency with which providers asked for patients' opinions and beliefs about their care improved in Kyaka II (2.84→3.28) and Kampala (3.27→3.48), reflecting the survivor-centred and participatory orientation reinforced through the inter-agency training. The stability of the indicator in Adjumani (3.22→3.19) — already higher at baseline — suggests baseline-saturation rather than weakening. Combined with the 100% post-training endorsement of relevance and improved capacity reported by the 40 inter-agency workshop participants, the survey confirms downstream effects on day-to-day service interactions.
KII/FGD Perspectives
Mainstreaming Quality and Rights into Frontline Care The inter-agency training sessions successfully entrenched human rights, ecological sustainability, and Core Humanitarian Standards (CHS) within the practical routines of frontline workers. Qualitative discussions confirm that equipping staff with holistic methodologies—specifically the integration of MHPSS with physical healthcare and GBV response—drastically mitigated operational silos. Staff emerged from the workshops better prepared to handle complex, trauma-laden interactions without succumbing to burnout or causing secondary victimization. "After undergoing some trainings... we learnt how to schedule time... so that people don't have to wait for so long" (KII, Psychosocial Counselor, Kampala).
Enhancing Patient-Provider Dynamics This institutional recalibration translated directly into the endline survey’s observation of improved provider behaviour, particularly the increased frequency of seeking patient opinions. The trainings demanded a pivot from paternalistic medical delivery to participatory, survivor-centred accompaniment. Farmamundi leadership emphasized that inter-agency upskilling fundamentally smoothed referral transitions, saving critical time for patients navigating multiple organizations. "These trainings... help us to connect VHTs with, in terms of health to referrers, to the correct people in the correct time" (KII, Deputy Director, Farmamundi, Spain). By aligning AHA, EMESCO, and Farmamundi onto a singular, empathetic operational frequency, the project vastly improved the dignity and quality of the everyday refugee care experience.
Activity 4.6. External Evaluation and External Audit
This activity was initiated during the reporting period and aimed to strengthen independent assessment, accountability, learning, transparency, and institutional compliance regarding project implementation and utilization of resources. As a process activity, it is not measured by a dedicated logframe indicator; the participation and feedback indicators reported under Activity 4.2 (I.O.V.1.R.4 and I.O.V.2.R.4) already capture stakeholder engagement, while the external evaluation and audit provide independent assurance over technical performance and financial management.
The ongoing external evaluation and audit processes further strengthens accountability, institutional learning, and transparency while contributing to broader reflection regarding project effectiveness, sustainability, and lessons learned that will inform the design of follow-on interventions.
Baseline/Endline Changes
While the external evaluation and audit are process activities not directly measured by the household survey, the broader accountability indicators tracked between baseline and endline — awareness of mechanisms (notable Kampala gain 66.7%→89.2%), feedback receipt across all sites, and improved patient–provider interaction ratings — provide an evidence base that supports the conclusions of the external evaluation: that accountability and Core Humanitarian Standards (CHS) practices have measurably strengthened, with the most pronounced gains in Kampala, partial gains in Adjumani, and remaining communication and visibility gaps in Kyaka II that the sustainability plan should address.
KII/FGD Perspectives
Enshrining Institutional Transparency and Learning The qualitative data showcases a profound appreciation for the stringent external assessment and auditing frameworks that governed the project. Implementing partners, RWCs, and Farmamundi leadership uniformly cited that frequent, transparent reporting back to the rights holders validated the consortium’s commitment to honesty. The regular rhythm of accountability meetings ensured that the project maintained agility, adapting to real-time communal friction. Farmamundi’s Deputy Director emphasized the rigorous institutional oversight: "Every month, we have an external audit that check everything" (KII, Deputy Director, Farmamundi, Spain).
Continuous Cycles of Participatory Improvement These final feedback sessions and independent evaluations were not viewed as punitive, but rather as essential compasses for future funding bids. Local stakeholders in Adjumani and Kyaka II enthusiastically embraced the endline evaluations as platforms to voice unvarnished needs regarding transitioning from emergency relief to sustainable livelihoods. A paralegal officer captured the forward-looking utility of these exercises: "This evaluation is going to help us to reinform us on what is currently happening... it's going to help us in our planning for our next project" (KII, Paralegal Officer, EMESCO, Adjumani). Ultimately, embedding external audits and extensive community feedback loops met the project's CHS mandates, leaving a blueprint for a highly accountable humanitarian architecture.